

Conventional versus miniaturized cardiopulmonary bypass: A systematic review and meta-analysis
- PMID: 36004169
- PMCID: PMC9390465
- DOI: 10.1016/j.xjon.2021.09.037
Conventional versus miniaturized cardiopulmonary bypass: A systematic review and meta-analysis
Abstract
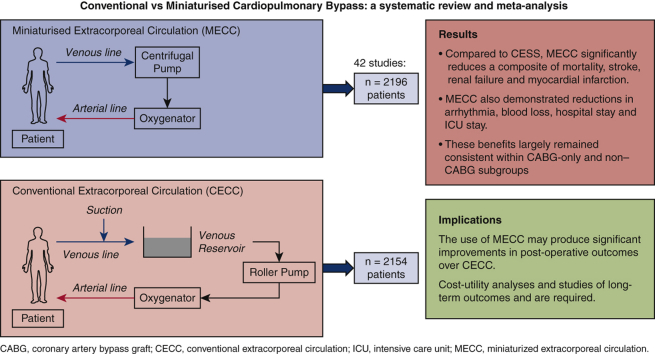
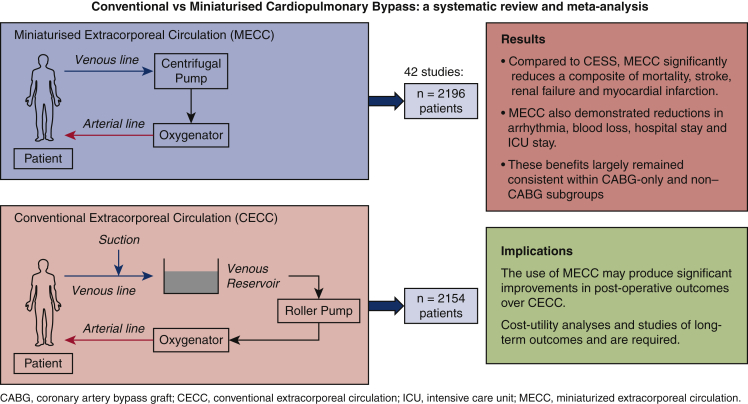
Objective: A meta-analysis of randomized controlled trials was performed to compare the effects of miniaturized extracorporeal circulation (MECC) and conventional extracorporeal circulation (CECC) on morbidity and mortality rates after cardiac surgery.
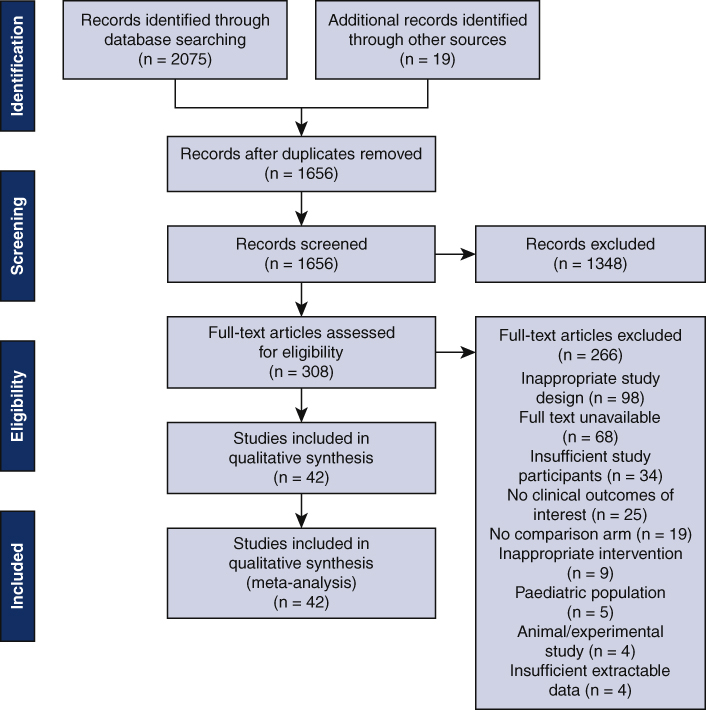
Methods: A comprehensive literature search was conducted using Ovid, PubMed, Medline, EMBASE, and the Cochrane databases. Randomized controlled trials from the year 2000 with n > 40 patients were considered. Key search terms included variations of "mini," "cardiopulmonary," "bypass," "extracorporeal," "perfusion," and "circuit." Studies were assessed for bias using the Cochrane Risk of Bias tool. The primary outcomes were postoperative mortality and stroke. Secondary outcomes included arrhythmia, myocardial infarction, renal failure, blood loss, and a composite outcome comprised of mortality, stroke, myocardial infarction and renal failure. Duration of intensive care unit, and hospital stay was also recorded.
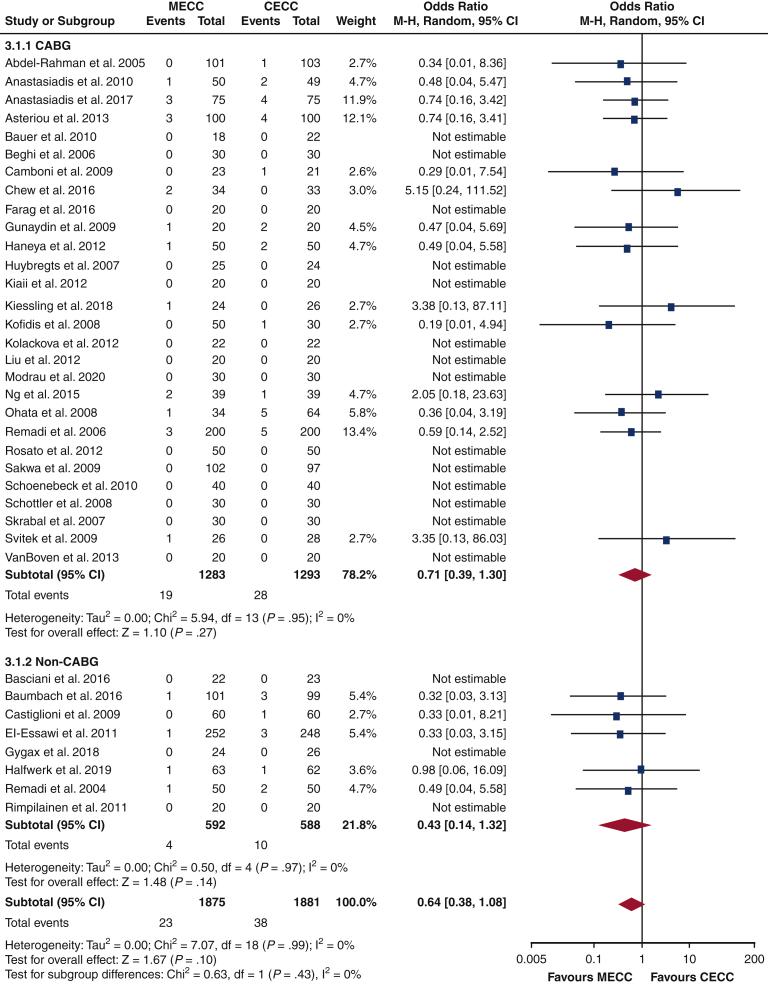
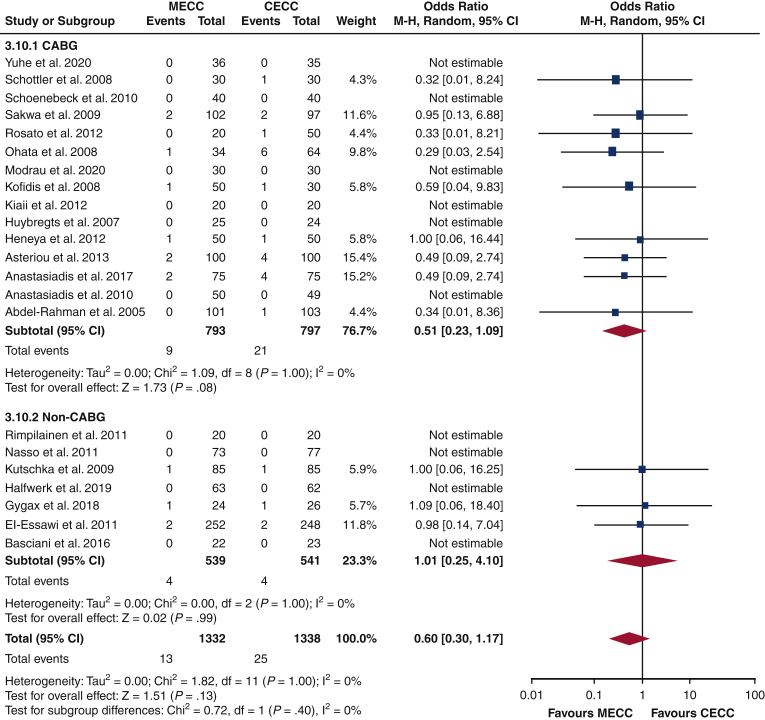
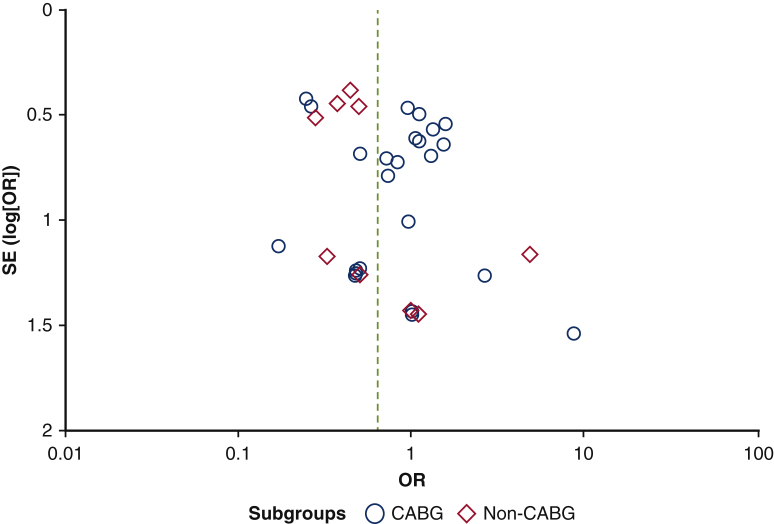
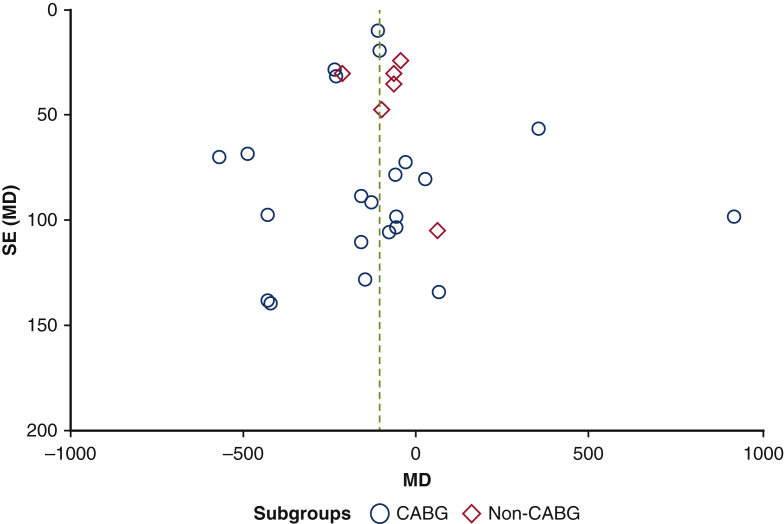
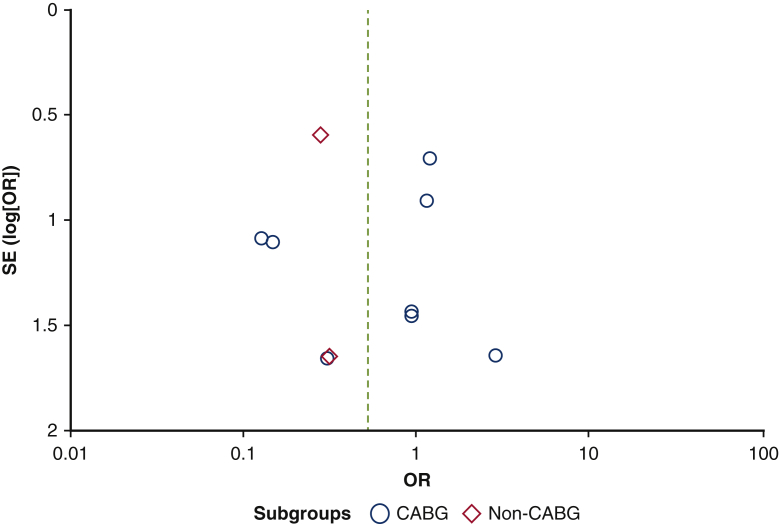
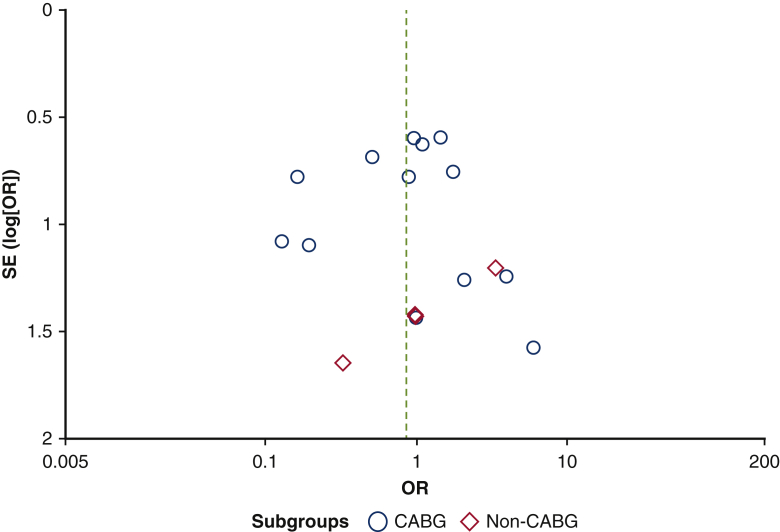
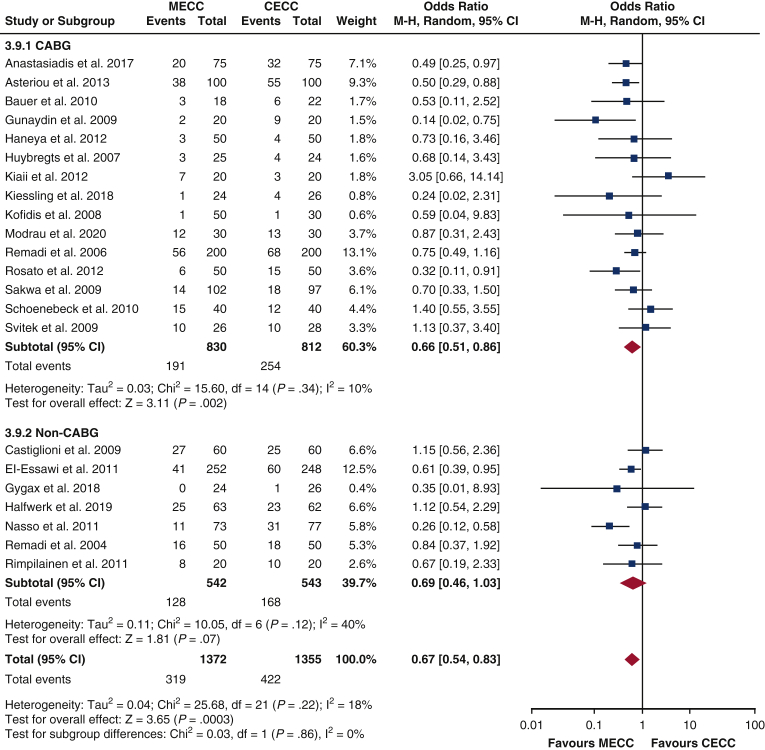
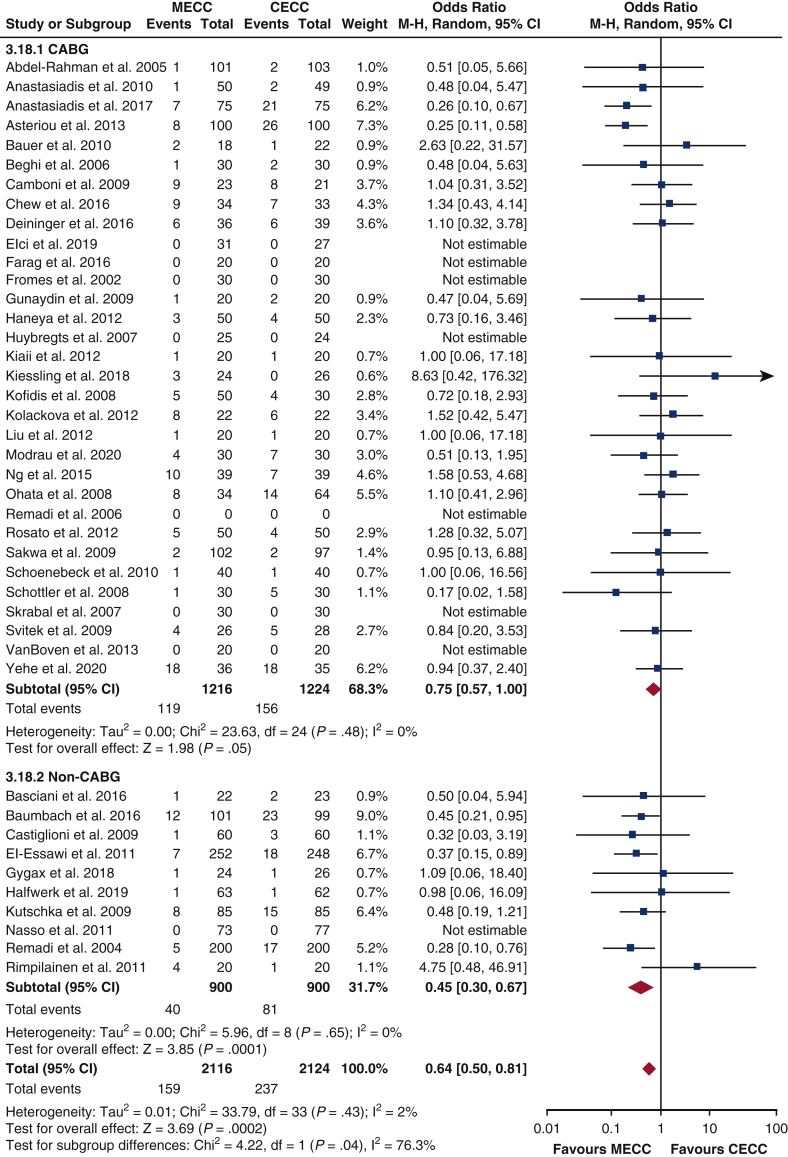
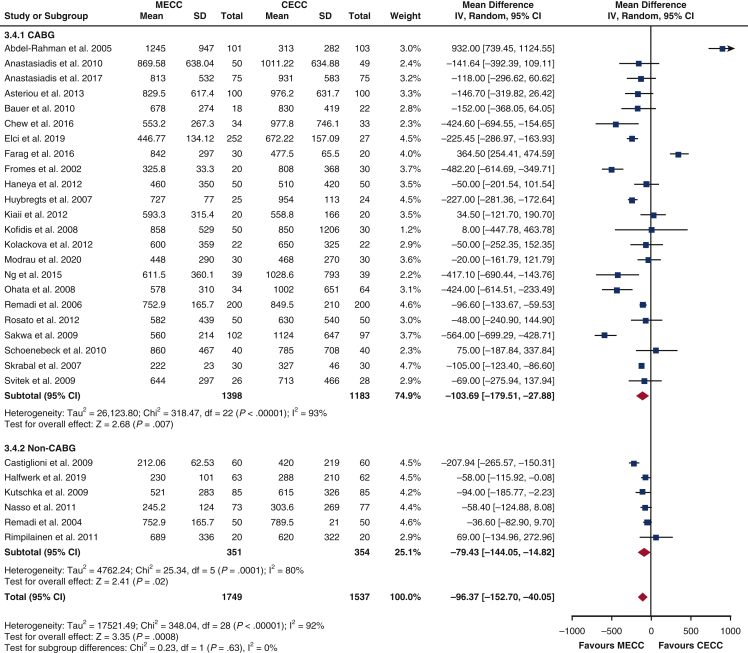
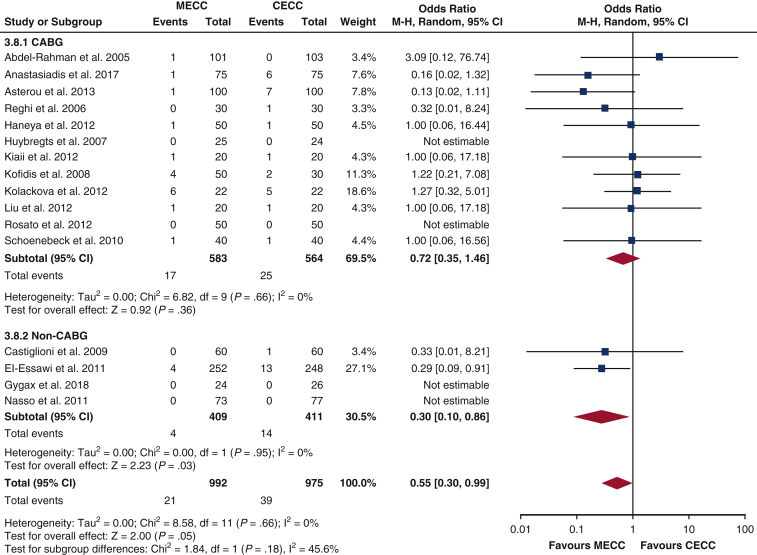
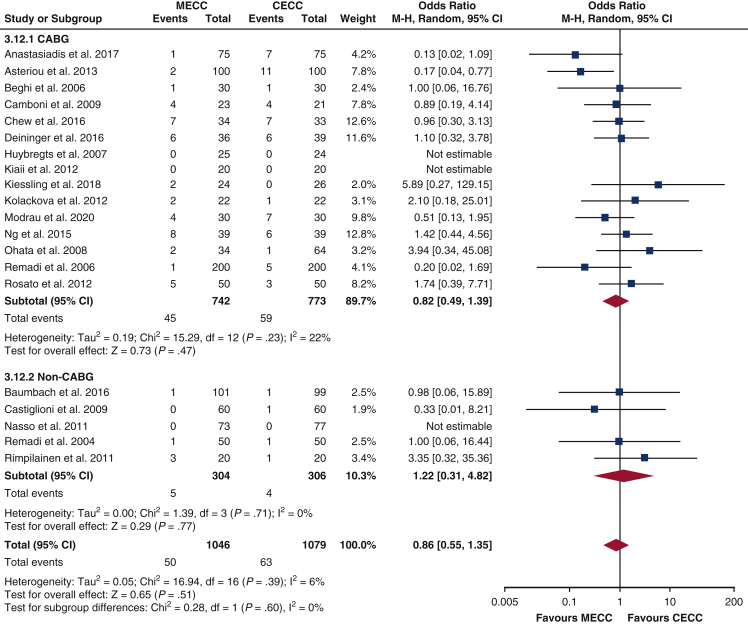
Results: The 42 studies eligible for this study included a total of 2154 patients who underwent CECC and 2196 patients who underwent MECC. There were no significant differences in any preoperative or demographic characteristics. Compared with CECC, MECC did not reduce the incidence of mortality, stroke, myocardial infarction, and renal failure but did significantly decrease the composite of these outcomes (odds ratio, 0.64; 95% confidence interval [CI], 0.50-0.81; P = .0002). MECC was also associated with reductions in arrhythmia (odds ratio, 0.67; 95% CI, 0.54-0.83; P = .0003), blood loss (mean difference [MD], -96.37 mL; 95% CI, -152.70 to -40.05 mL; P = .0008), hospital stay (MD, -0.70 days; 95% CI, -1.21 to -0.20 days; P = .006), and intensive care unit stay (MD, -2.27 hours; 95% CI, -3.03 to -1.50 hours; P < .001).
Conclusions: MECC demonstrates clinical benefits compared with CECC. Further studies are required to perform a cost-utility analysis and to assess the long-term outcomes of MECC. These should use standardized definitions of endpoints such as mortality and renal failure to reduce inconsistency in outcome reporting.
Keywords: AKI, acute kidney injury; CABG, coronary artery bypass graft; CECC, conventional extracorporeal circulation; CI, confidence interval; CPB, cardiopulmonary bypass; FFP, fresh-frozen plasma; ICU, intensive care unit; IL-6, interleukin-6; IL-8, interleukin-8; MECC, miniaturized extracorporeal circulation; MI, myocardial infarction; OR, odds ratio; POAF, postoperative atrial fibrillation; RBC, red blood cells; RCT, randomized control trial; cardiac surgery; cardiopulmonary bypass; coronary-artery bypass grafting; meta-analysis; minimal extracorporeal circulation.
© 2021 The Author(s).
Figures
References
-
- Zangrillo A., Garozzo F.A., Biondi-Zoccai G., Pappalardo F., Monaco F., Crivellari M., et al. Miniaturized cardiopulmonary bypass improves short-term outcome in cardiac surgery: a meta-analysis of randomized controlled studies. J Thorac Cardiovasc Surg. 2010;139:1162–1169. - PubMed
-
- Paparella D., Yau T.M., Young E. Cardiopulmonary bypass induced inflammation: pathophysiology and treatment. An update. Eur J Cardiothorac Surg. 2002;21:232–244. - PubMed
-
- Westaby S. Organ dysfunction after cardiopulmonary bypass. A systemic inflammatory reaction initiated by the extracorporeal circuit. Intensive Care Med. 2021;13:89–95. - PubMed
-
- Savageau J.A., Stanton B.A., Jenkins C.D., Frater R.W. Neuropsychological dysfunction following elective cardiac operation. II. A six-month reassessment. J Thorac Cardiovasc Surg. 1982;84:595–600. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
