

Select octogenarians with stage IIIa non-small cell lung cancer can benefit from trimodality therapy
- PMID: 36004217
- PMCID: PMC9390188
- DOI: 10.1016/j.xjon.2022.01.022
Select octogenarians with stage IIIa non-small cell lung cancer can benefit from trimodality therapy
Abstract
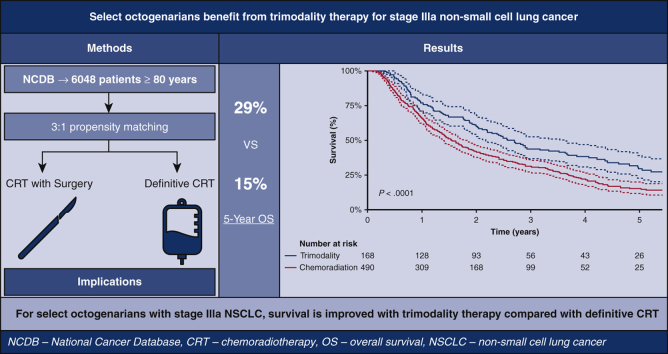
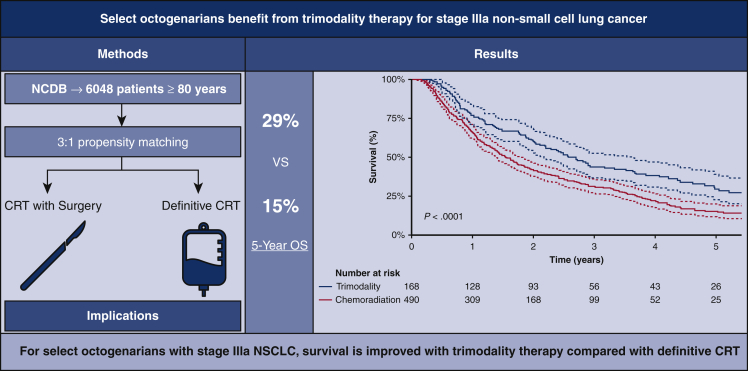
Objectives: Currently, more than 36% of patients diagnosed with lung cancer are 75 years of age or older. Management of stage IIIA cancer is variable, especially for octogenarians who might not be offered surgery because of questionable benefit. In this study we investigated the outcomes of definitive chemoradiotherapy (CR) and trimodality therapy (TM) management (CR and surgery) for clinical stage IIIA non-small cell lung cancer (NSCLC) in patients 80 years of age or older.
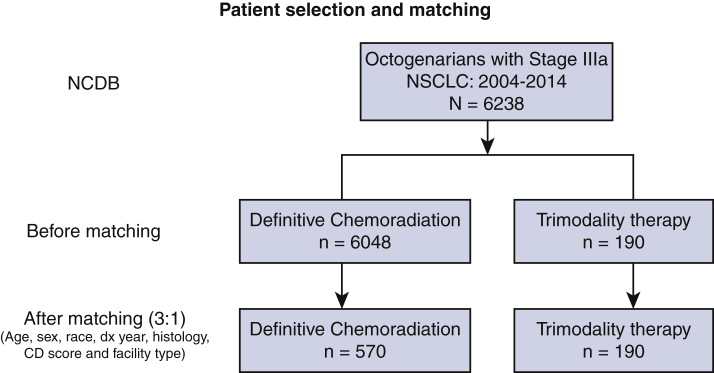
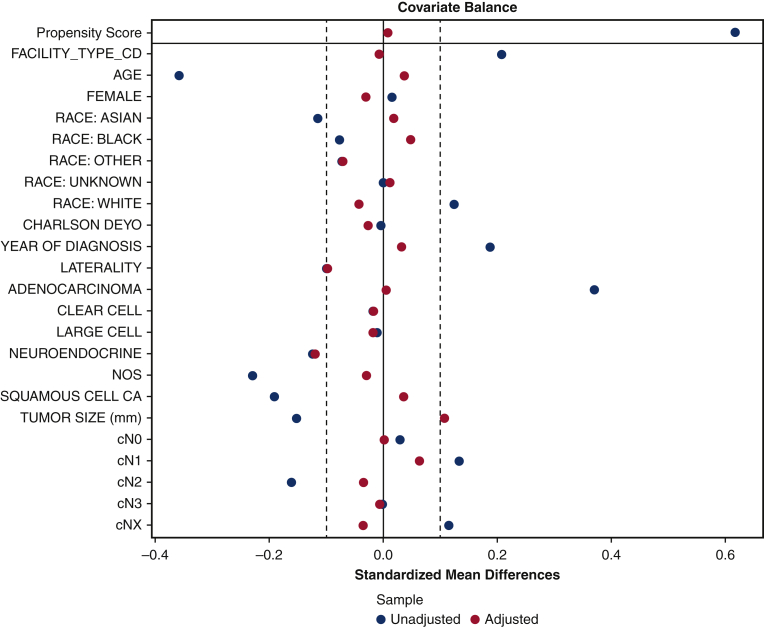
Methods: The National Cancer Data Base was queried for stage IIIA NSCLC in patients 80 years of age or older between 2004 and 2015. Patients were divided according to treatment type: definitive CR and TM. Patient demographic characteristics, facility type, Charlson-Deyo score, final tumor pathology, and survival data were extracted. Univariate analysis was performed, followed by 3:1 propensity matching to analyze overall survival differences. Unadjusted and adjusted Kaplan-Meier survival analyses were performed.
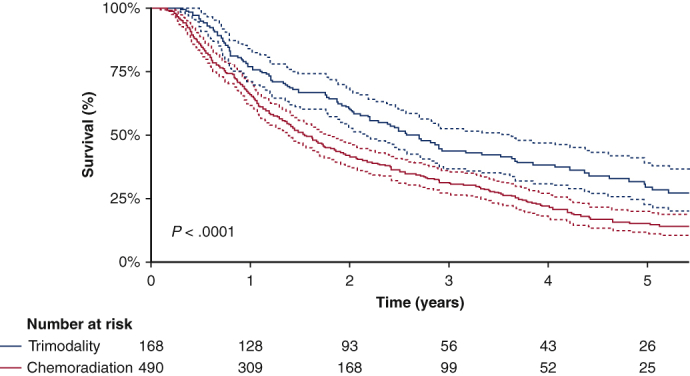
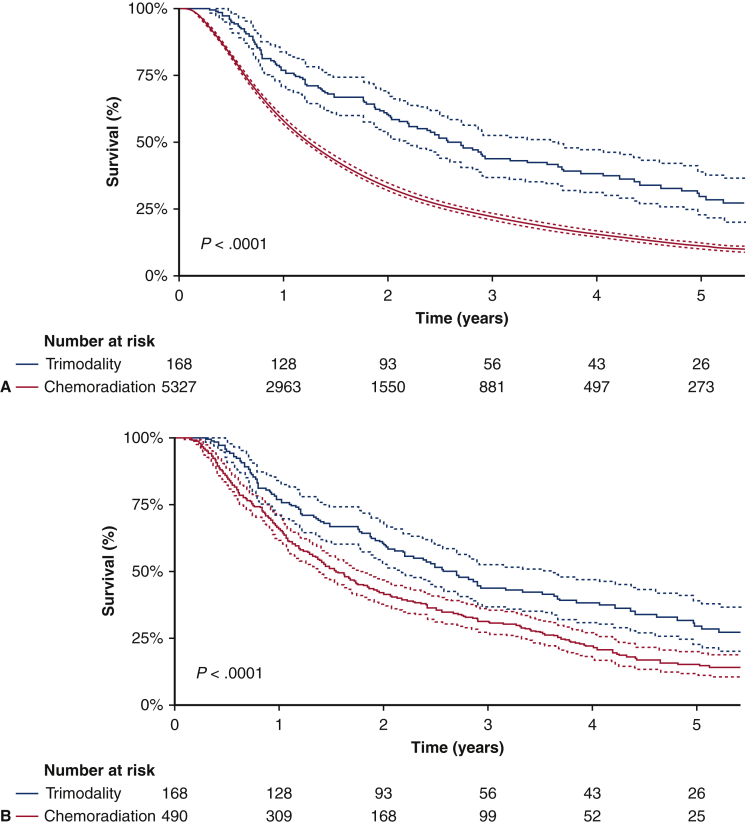
Results: From the database, 6048 CR and 190 TM octogenarians were identified. Patients in the TM group were younger (82 years old [TM] vs 83 years old [CR]; P < .0001), more likely to be treated at an academic/research institution (36% [TM] vs 26% [CR]; P = .003), had greater proportion of adenocarcinoma (52% [TM] vs 34% [CR]; P < .001), and a smaller tumor size (38 mm [TM] vs 33 mm [CR]; P = .025). After 3:1 matching, the 5-year overall survival for the TM group was 29% (95% CI, 22%-38%) versus 15% (95% CI, 11%-20%) for the CR group.
Conclusions: Selected elderly patients with stage IIIa NSCLC can benefit from an aggressive TM approach.
Keywords: CR, chemoradiotherapy; NCDB, National Cancer Database; NSCLC; NSCLC, non–small cell lung cancer; TM, trimodality therapy; octogenarian; stage IIIa; trimodality therapy.
© 2022 The Author(s).
Figures
Similar articles
-
Importance of tumour volume and histology in trimodality treatment of patients with Stage IIIA non-small cell lung cancer-results from a retrospective analysis.Interact Cardiovasc Thorac Surg. 2022 Mar 31;34(4):566-575. doi: 10.1093/icvts/ivab291. Interact Cardiovasc Thorac Surg. 2022. PMID: 34734237 Free PMC article.
-
Trimodality therapy for stage IIIA non-small cell lung cancer: benchmarking multi-disciplinary team decision-making and function.Lung Cancer. 2014 Aug;85(2):218-23. doi: 10.1016/j.lungcan.2014.06.005. Epub 2014 Jun 16. Lung Cancer. 2014. PMID: 24976333
-
Trimodality vs Chemoradiation and Salvage Resection in cN2 Stage IIIA Non-Small Cell Lung Cancer.Semin Thorac Cardiovasc Surg. 2020 Spring;32(1):153-159. doi: 10.1053/j.semtcvs.2019.06.002. Epub 2019 Jun 17. Semin Thorac Cardiovasc Surg. 2020. PMID: 31220530 Free PMC article.
-
Role of Postoperative Radiotherapy in Pathologic Stage IIIA (N2) Non-Small Cell Lung Cancer in a Prospective Nationwide Oncology Outcomes Database.J Thorac Oncol. 2017 Feb;12(2):302-313. doi: 10.1016/j.jtho.2016.09.135. Epub 2016 Oct 14. J Thorac Oncol. 2017. PMID: 27746190
-
Treatment-Related Predictive and Prognostic Factors in Trimodality Approach in Stage IIIA/N2 Non-Small Cell Lung Cancer.Front Oncol. 2018 Feb 20;8:30. doi: 10.3389/fonc.2018.00030. eCollection 2018. Front Oncol. 2018. PMID: 29527511 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
