

Early and late outcomes of type A acute aortic dissection with common carotid artery involvement
- PMID: 36004235
- PMCID: PMC9390160
- DOI: 10.1016/j.xjon.2022.01.024
Early and late outcomes of type A acute aortic dissection with common carotid artery involvement
Abstract
Objective: The relationship between common carotid artery (CCA) involvement in acute type A aortic dissection (ATAAD) and postoperative outcomes remains unclear. We investigated outcomes and described our current advanced strategy.
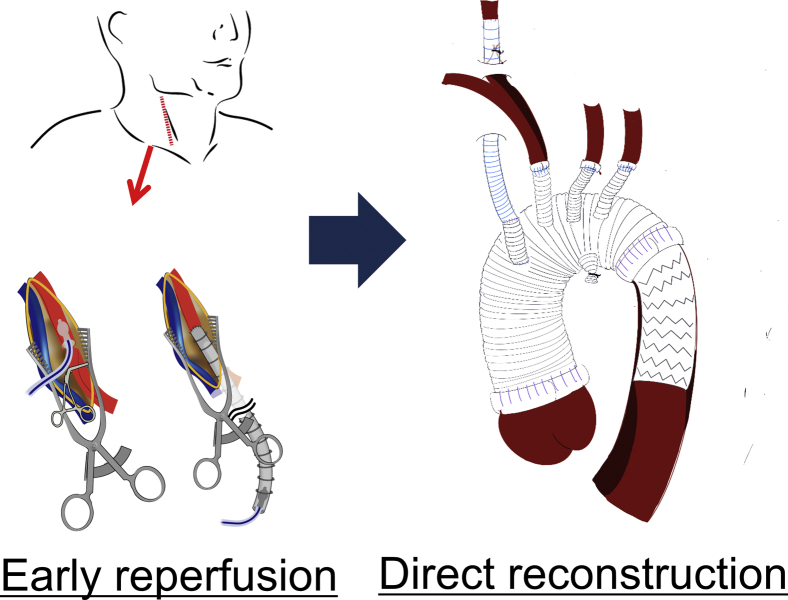
Methods: Of 492 patients who underwent surgical repair for ATAAD between September 1999 and February 2021, CCA involvement was identified in 114. Eighty of these 114 patients (70.2%) were classified as having a thrombosed CCA and 34 (29.8%) were classified as nonthrombosed. To prevent postoperative cerebral malperfusion, we initiated a strategy of early reperfusion and direct reconstruction of dissected and thrombosed CCAs regardless of neurologic symptoms.
Results: Fifty-five patients (48.2%) showed preoperative neurologic symptoms. No significant differences between the thrombosed and nonthrombosed groups were seen in postoperative mortality (20.0% vs 11.8%; P = .421) or frequency of postoperative modified Rankin scale (mRS) score ≥5 (30.0% vs 17.6%; P = .245). The rate of postoperative neurologic deficit was significantly higher (48.8% vs 23.5%; P = .013) and long-term survival rate was significantly lower (5 years; 59.1 ± 6.3% vs 77.9 ± 7.4%; 10 years: 50.0 ± 7.9% vs 72.3 ± 8.7%; P = .041) in the thrombosed group. Risk factors for mRS ≥5 from multivariable analysis included occluded thrombosed CCA, preoperative coma, preoperative shock, and prolonged operation time. Fifteen patients were treated with the early reperfusion and direct reconstruction strategy; postoperative mortality 13.3% (2 patients). No patients showed cerebral reperfusion syndrome.
Conclusions: In patients with CCA involvement, a thrombosed false lumen, especially an occluded CCA, resulted in worse outcomes regardless of preoperative neurologic symptoms. Further study is needed to evaluate the efficacy of the current strategy.
Keywords: ATAAD, acute type A aortic dissection; BSS, brain-saving system; CCA, common carotid artery; CT, computed tomography; ICA, internal carotid artery; IQR, interquartile range; PND, persistent neurologic deficit; TND, transient neurologic deficit; aortic dissection; carotid artery; cerebral perfusion; mRS, modified Rankin scale; malperfusion syndrome; stroke.
© 2022 The Author(s).
Figures






References
-
- Okita Y., Kumamaru H., Motomura N., Miyata H., Takamoto S. Current status of open surgery for acute type A aortic dissection in Japan. J Thorac Cardiovasc Surg. November 11, 2020 [Epub ahead of print] - PubMed
-
- Committee for Scientific Affairs, The Japanese Association for Thoracic Surgery. Shimizu H., Okada M., Toh Y., Doki Y., Endo S., Fukuda H., et al. Thoracic and cardiovascular surgeries in Japan during 2018: annual report by the Japanese association for thoracic surgery. Gen Thorac Cardiovasc Surg. 2021;69:179–212. - PMC - PubMed
-
- Tanaka H., Okada K., Yamashita T., Morimoto Y., Kawanishi Y., Okita Y. Surgical results of acute aortic dissection complicated with cerebral malperfusion. Ann Thorac Surg. 2005;80:72–76. - PubMed
-
- Bossone E., Corteville D.C., Harris K.M., Suzuki T., Fattori R., Hutchison S., et al. Stroke and outcomes in patients with acute type A aortic dissection. Circulation. 2013;128(11Suppl 1):S175–S179. - PubMed
-
- Sultan I., Bianco V., Patel H.J., Arnaoutakis G.J., Di Eusanio M., Chen E.P., et al. Surgery for type A aortic dissection in patients with cerebral malperfusion: results from the International registry of acute aortic dissection. J Thorac Cardiovasc Surg. 2019;161:1713–1720.e1. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
