

Silent cerebral ischemia detected by magnetic resonance imaging can predict postoperative delirium after total arch replacement for aneurysm
- PMID: 36004275
- PMCID: PMC9390522
- DOI: 10.1016/j.xjon.2022.02.026
Silent cerebral ischemia detected by magnetic resonance imaging can predict postoperative delirium after total arch replacement for aneurysm
Abstract
Objective: To identify whether preoperative magnetic resonance imaging findings of the brain can predict postoperative delirium in patients who undergo arch replacement for aneurysms.
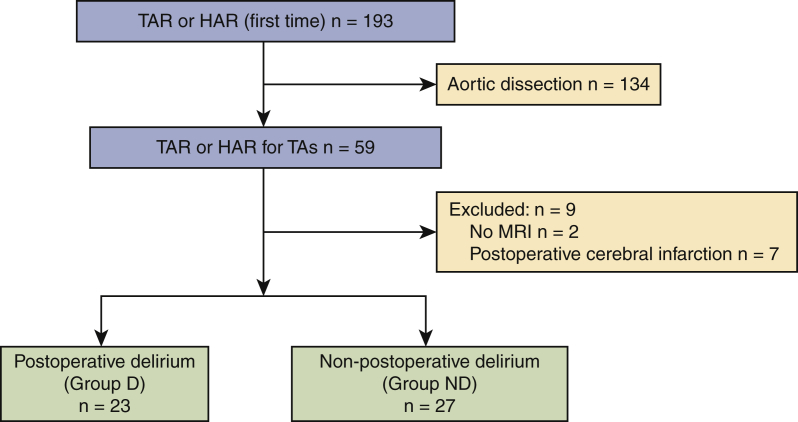
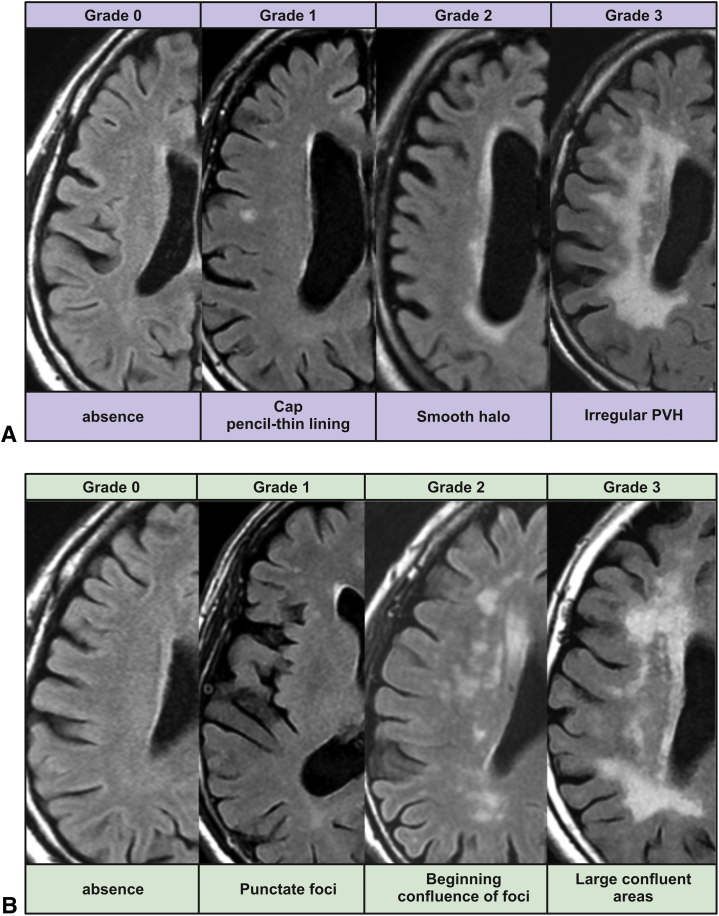
Methods: Overall, 193 patients who underwent aortic replacement for the first time at a single institution between April 2014 and September 2020 were enrolled in this retrospective study. After we excluded patients with acute aortic dissection, no preoperative magnetic resonance imaging findings of the brain, and postoperative cerebral infarction, 50 patients were included and divided into 2 groups, according to their confusion scale results: postoperative delirium (group D) and nonpostoperative delirium (group ND). Preoperative magnetic resonance imaging findings of the brain were classified into lacunar stroke, periventricular hyperintensity, and deep subcortical white matter hyperintensity groups; the latter 2 groups were further classified based on the Fazekas scale, grade 0 to 3.
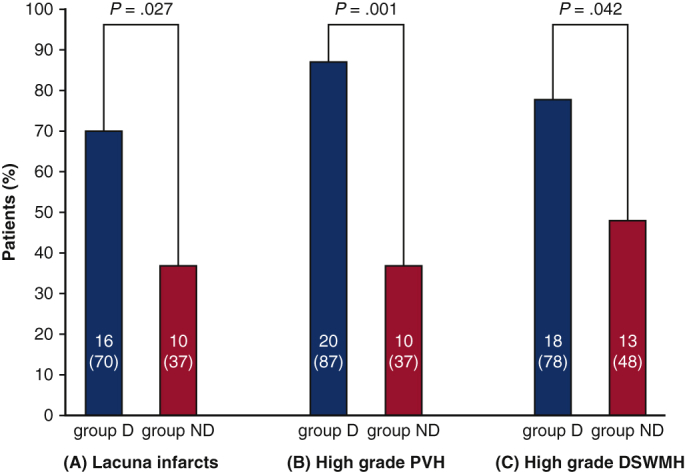
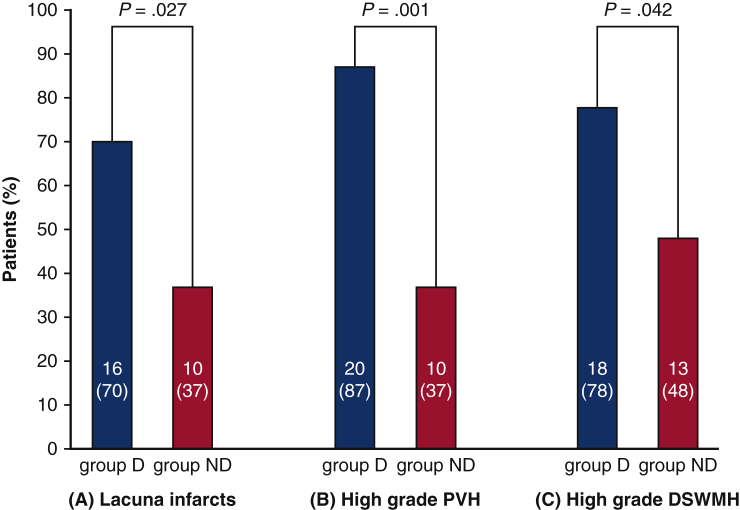
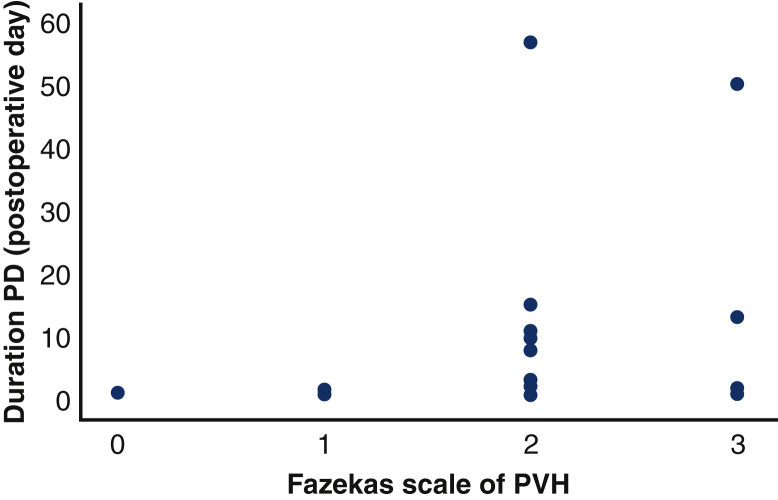
Results: There were 23 patients (46%) in group D and 27 (54%) in group ND. The mean age was significantly greater in group D than in group ND (75 vs 70 years; P = .007). The mean operative time was significantly longer in group D than in group ND (447 vs 384 minutes; P = .024). As for preoperative magnetic resonance imaging findings of the brain, there were significantly more lacunar stroke cases in group D than in group ND (P = .027). In multivariable logistic regression with stepwise selection, high-grade periventricular hyperintensity was significantly related to postoperative delirium (odds ratio, 9.38; 95% confidence interval, 1.55-56.56; P = .015).
Conclusions: Silent cerebral ischemia detected by preoperative magnetic resonance imaging of the brain was a significant risk factor for postoperative delirium.
Keywords: AAA, aortic arch aneurysm; AR, arch replacement; CI, confidence interval; DSWMH, deep subcortical white matter hyperintensities; ICDSC, Intensive Care Delirium Screening Checklist; ICU, intensive care unit; MRI, magnetic resonance imaging; NCS, Neelon and Champagne confusion scale; NPD, nonpostoperative delirium; OR, odds ratio; PD, postoperative delirium; PVH, periventricular hyperintensity; SCP, selective cerebral perfusion; TAR, total arch replacement; TEVAR, thoracic endovascular aortic repair; WMH, white matter hyperintensity; magnetic resonance imaging; postoperative delirium; total arch replacement; white matter intensity.
© 2022 The Author(s).
Figures


Similar articles
-
Prevalence of carotid artery stenosis and intra-cranial lesions in patients with aortic arch aneurysm and its association with intraoperative regional cerebral oxygen saturation and postoperative neurological outcomes.J Thorac Dis. 2024 May 31;16(5):2713-2722. doi: 10.21037/jtd-24-78. Epub 2024 May 24. J Thorac Dis. 2024. PMID: 38883627 Free PMC article.
-
Mortality and cerebral outcome in patients who underwent aortic arch operations using deep hypothermic circulatory arrest with retrograde cerebral perfusion: no relation of early death, stroke, and delirium to the duration of circulatory arrest.J Thorac Cardiovasc Surg. 1998 Jan;115(1):129-38. doi: 10.1016/s0022-5223(98)70451-9. J Thorac Cardiovasc Surg. 1998. PMID: 9451056
-
Silent cerebral infarction after thoracic endovascular aortic repair: a magnetic resonance imaging study.Eur J Cardiothorac Surg. 2019 Jun 1;55(6):1071-1078. doi: 10.1093/ejcts/ezy449. Eur J Cardiothorac Surg. 2019. PMID: 30629169
-
Preoperative brain magnetic resonance imaging and postoperative delirium after off-pump coronary artery bypass grafting: a prospective cohort study.Can J Anaesth. 2015 Jun;62(6):595-602. doi: 10.1007/s12630-015-0327-x. Epub 2015 Feb 5. Can J Anaesth. 2015. PMID: 25652160
-
Endovascular stent grafting and open surgical replacement for chronic thoracic aortic aneurysms: a systematic review and prospective cohort study.Health Technol Assess. 2022 Jan;26(6):1-166. doi: 10.3310/ABUT7744. Health Technol Assess. 2022. PMID: 35094747
Cited by
-
Infarct-related structural disconnection and delirium in surgical aortic valve replacement patients.Ann Clin Transl Neurol. 2024 Feb;11(2):263-277. doi: 10.1002/acn3.51949. Epub 2023 Dec 28. Ann Clin Transl Neurol. 2024. PMID: 38155462 Free PMC article. Clinical Trial.
-
Post-anesthesia care unit delirium in children with moyamoya disease undergoing indirect revascularization: incidence and risk factors.Korean J Anesthesiol. 2025 Apr;78(2):129-138. doi: 10.4097/kja.24481. Epub 2024 Dec 20. Korean J Anesthesiol. 2025. PMID: 39703186 Free PMC article.
-
Prevalence of carotid artery stenosis and intra-cranial lesions in patients with aortic arch aneurysm and its association with intraoperative regional cerebral oxygen saturation and postoperative neurological outcomes.J Thorac Dis. 2024 May 31;16(5):2713-2722. doi: 10.21037/jtd-24-78. Epub 2024 May 24. J Thorac Dis. 2024. PMID: 38883627 Free PMC article.
-
Commentary: Sometimes it helps to take a closer look.JTCVS Open. 2022 Apr 19;10:99-100. doi: 10.1016/j.xjon.2022.04.014. eCollection 2022 Jun. JTCVS Open. 2022. PMID: 36004219 Free PMC article. No abstract available.
-
Commentary: Detailed assessment of hidden risks of postoperative delirium.JTCVS Open. 2022 Apr 19;10:97-98. doi: 10.1016/j.xjon.2022.04.021. eCollection 2022 Jun. JTCVS Open. 2022. PMID: 36004257 Free PMC article. No abstract available.
References
-
- Järvelä K., Porkkala H., Karlsson S., Martikainen T., Selander T., Bendel S. Postoperative delirium in cardiac surgery patients. J Cardiothorac Vasc Anesth. 2018;32:1597–1602. - PubMed
-
- Habeeb-Allah A., Alshraideh J.A. Delirium post-cardiac surgery: incidence and associated factors. Nurs Crit Care. 2021;26:150–155. - PubMed
-
- Sugimura Y., Sipahi N.F., Mehdiani A., Petrov G., Awe M., Minol J.P., et al. Risk and consequences of postoperative delirium in cardiac surgery. Thorac Cardiovasc Surg. 2020;68:417–424. - PubMed
-
- Krzych L.J., Wybraniec M.T., Krupka-Matuszczyk I., Skrzypek M., Bolkowska A., Wilczyński M., et al. Detailed insight into the impact of postoperative neuropsychiatric complications on mortality in a cohort of cardiac surgery subjects: a 23,000-patient-year analysis. J Cardiothorac Vasc Anesth. 2014;28:448–457. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
