

A Nonrestrictive Approach to Fluoroquinolone Stewardship at Two Community Hospitals
- PMID: 36004311
- PMCID: PMC9394769
- DOI: 10.1093/ofid/ofac388
A Nonrestrictive Approach to Fluoroquinolone Stewardship at Two Community Hospitals
Abstract
Background: Fluoroquinolones are one of the most prescribed antimicrobials in the United States and have been increasingly used in inpatient and outpatient settings to treat various infectious diseases syndromes. Due to the unwanted collateral effects on antibiotic resistance, poor susceptibility rates among Gram-negative pathogens, and adverse effects, fluoroquinolones are often targeted by hospital antimicrobial stewardship programs to prevent overutilization. This study describes the association of nonrestrictive antimicrobial stewardship interventions at 2 nonacademic community hospitals on levofloxacin utilization, prescribing patterns on alternative antibiotics, and Pseudomonas aeruginosa nonsusceptibility rates to levofloxacin.
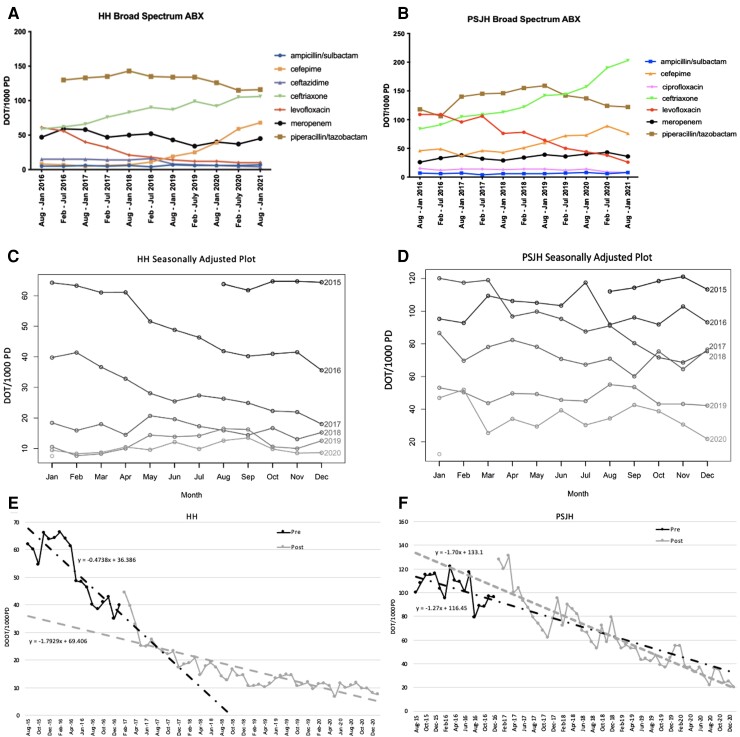
Methods: Nonrestrictive antimicrobial stewardship interventions included monitoring and reporting of fluoroquinolone susceptibility trends to physician groups, performing medication use evaluations of levofloxacin accompanied with prescriber detailing, daily prospective audit and feedback, implementation of beta-lactam-based institutional guidelines for empiric therapy in various infectious disease syndromes, review and adjustment of electronic medical record order sets containing fluoroquinolones, and intensive prescriber education. No preauthorization of levofloxacin was used during this study period. Antibiotic utilization data were collected for the time periods of August 2015 through January 2021. Correlation between levofloxacin and other broad-spectrum antibiotc use was investigated as well as the impact on Pseudomonas aeruginosa levofloxacin nonsusceptibility rates.
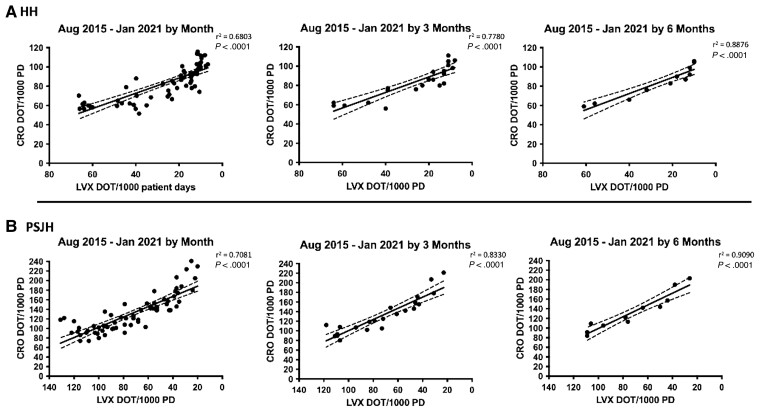
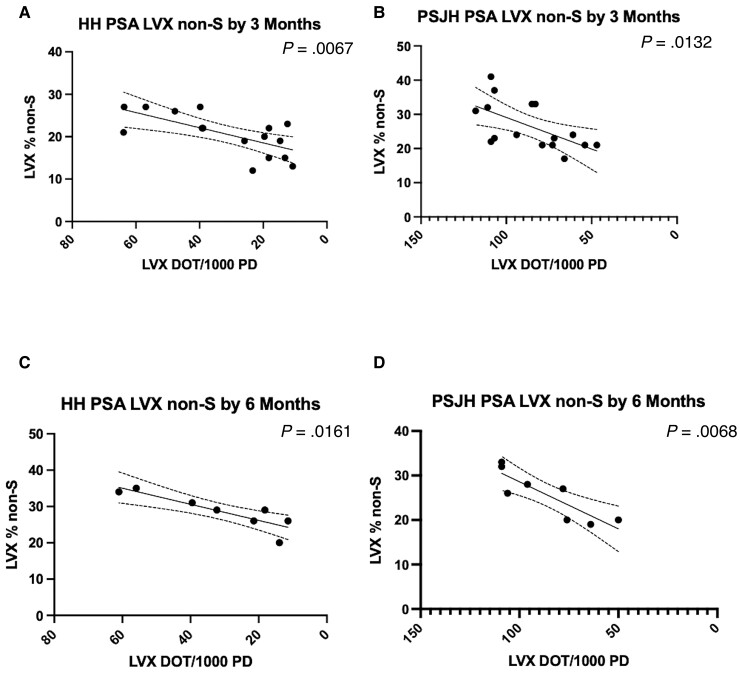
Results: Both hospitals showed an overall downward trend in the prescribing of levofloxacin during the time period of August 2015 to January 2021. There was a significant negative correlation between monthly ceftriaxone and levofloxacin days of therapy for both hospitals (P < .0001). There was a positive correlation between levofloxacin days of therapy and P aeruginosa nonsusceptibility (P < .02 at both hospitals).
Conclusions: Our results demonstrate that a nonrestrictive approach to fluoroquinolone stewardship interventions had a significant impact on reducing levofloxacin utilization, increasing ceftriaxone utilization, and improving P aeruginosa levofloxacin susceptibility.
Keywords: antibiotic stewardship; antimicrobial resistance; antimicrobial stewardship program; fluoroquinolone stewardship; levofloxacin.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
Similar articles
-
The Association of Antibiotic Stewardship With Fluoroquinolone Prescribing in Michigan Hospitals: A Multi-hospital Cohort Study.Clin Infect Dis. 2019 Sep 27;69(8):1269-1277. doi: 10.1093/cid/ciy1102. Clin Infect Dis. 2019. PMID: 30759198 Free PMC article.
-
Short- and long-term impact of a multifaceted approach targeting fluoroquinolone use in a community hospital: an interrupted time-series analysis.Int J Clin Pharm. 2022 Jun;44(3):741-748. doi: 10.1007/s11096-022-01405-8. Epub 2022 Apr 21. Int J Clin Pharm. 2022. PMID: 35451671
-
Evaluation of a carbapenem antimicrobial stewardship program and clinical outcomes in a Japanese hospital.J Infect Chemother. 2022 Jul;28(7):884-889. doi: 10.1016/j.jiac.2022.03.006. Epub 2022 Mar 21. J Infect Chemother. 2022. PMID: 35331613
-
Review of antimicrobial resistance control strategies: low impact of prospective audit with feedback on bacterial antibiotic resistance within hospital settings.Infect Dis (Lond). 2021 Mar;53(3):159-168. doi: 10.1080/23744235.2020.1846777. Epub 2020 Dec 10. Infect Dis (Lond). 2021. PMID: 33300825 Review.
-
Antimicrobial Stewardship Interventions to Combat Antibiotic Resistance: an Update on Targeted Strategies.Curr Infect Dis Rep. 2019 Aug 31;21(10):33. doi: 10.1007/s11908-019-0689-2. Curr Infect Dis Rep. 2019. PMID: 31473861 Review.
Cited by
-
Outpatient treatment of pneumonia in a setting with and without an infectious disease doctor.Croat Med J. 2023 Feb 28;64(1):45-51. doi: 10.3325/cmj.2023.64.45. Croat Med J. 2023. PMID: 36864818 Free PMC article.
References
-
- Linder JA, Huang ES, Steinman MA, Gonzales R, Stafford RS. Fluoroquinolone prescribing in the United States: 1995 to 2002. Am J Med 2005; 118:259–68. - PubMed
-
- Adam HJ, Hoban DJ, Gin AS, Zhanel GG. Association between fluoroquinolone usage and a dramatic rise in ciprofloxacin-resistant Streptococcus pneumoniae in Canada, 1997–2006. Int J Antimicrob Agents 2009; 34:82–5. - PubMed
-
- Lee YJ, Liu HY, Lin YC, Sun KL, Chun CL, Hsueh PR. Fluoroquinolone resistance of Pseudomonas aeruginosa isolates causing nosocomial infection is correlated with levofloxacin but not ciprofloxacin use. Int J Antimicrob Agents 2010; 35:261–4. - PubMed
