

High-flow nasal oxygen reduces the incidence of hypoxia in sedated hysteroscopy for assisted reproduction
- PMID: 36004375
- PMCID: PMC9394211
- DOI: 10.3389/fmed.2022.929096
High-flow nasal oxygen reduces the incidence of hypoxia in sedated hysteroscopy for assisted reproduction
Abstract
Backgrounds and aims: Pain is the main reason for hysteroscopy failure. In day-surgical settings, hysteroscopy procedures are commonly performed with the patient under sedation. Hypoxia is the most common adverse event during sedation and can lead to severe adverse events. This study aimed to compare the incidence of hypoxia when using high-flow nasal oxygen (HFNO) with that when using regular nasal oxygen in patients undergoing hysteroscopy with sedation.
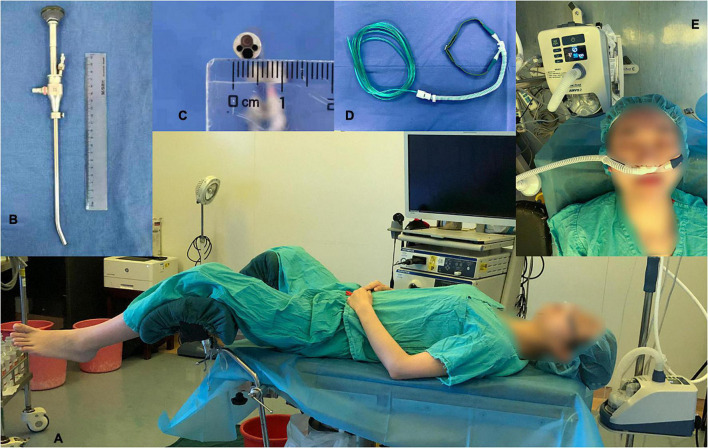
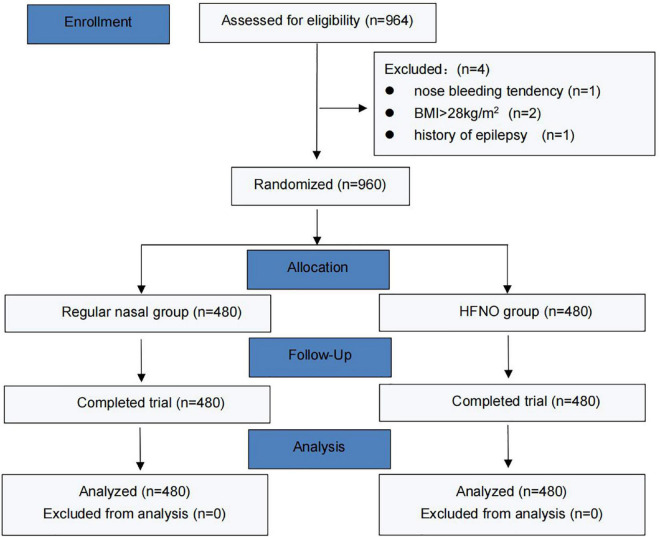
Materials and methods: In this single-center, prospective, randomized, single-blinded study, 960 female patients undergoing elective diagnostic or operative hysteroscopy were randomly enrolled into the following two groups: the regular nasal group [O2 (3-6 L/min) covered by an HFNO] and the HFNO group [O2 (30-60 L/min)] from September 2021 to December 2021. All women were sedated with propofol (1.5 mg/kg) and remifentanil (1.5 μg/kg) in the operating room. The primary outcome was the incidence of hypoxia (75% ≤ SpO2 < 90%, < 60 s).
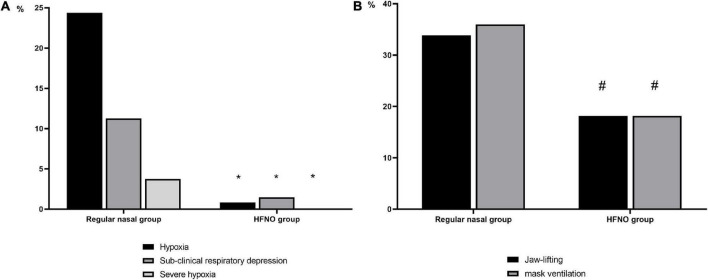
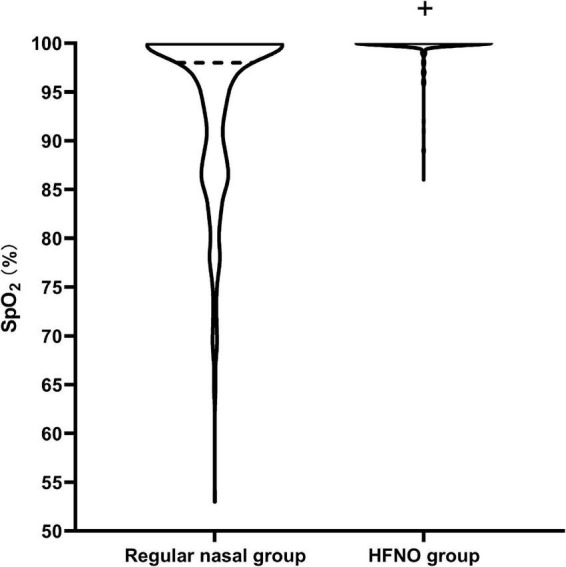
Results: HFNO decreased the incidence of hypoxia (75% ≤ SpO2 < 90%, < 60 s), subclinical respiratory depression (90% ≤ SpO2 < 95%) and severe hypoxia (SpO2 < 75% for any duration or 75% ≤ SpO2 < 90% for ≥ 60 s) from 24.38 to 0.83%, from 11.25 to 1.46% and from 3.75 to 0%, respectively (P < 0.001).
Conclusion: In procedures conducted to treat female infertility, HFNO can reduce hypoxia during hysteroscopy in patients sedated with propofol, and it can prevent the occurrence of subclinical respiratory depression and severe hypoxia.
Keywords: deep sedation; high-flow nasal oxygen; hypoxia; hysteroscopy; in vitro fertilization; propofol.
Copyright © 2022 Tang, Huang, Chai, Zhang, Zhang, Chen, Su and Huang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources