

COVID-19 induces CNS cytokine expression and loss of hippocampal neurogenesis
- PMID: 36004663
- PMCID: PMC9452175
- DOI: 10.1093/brain/awac270
COVID-19 induces CNS cytokine expression and loss of hippocampal neurogenesis
Abstract
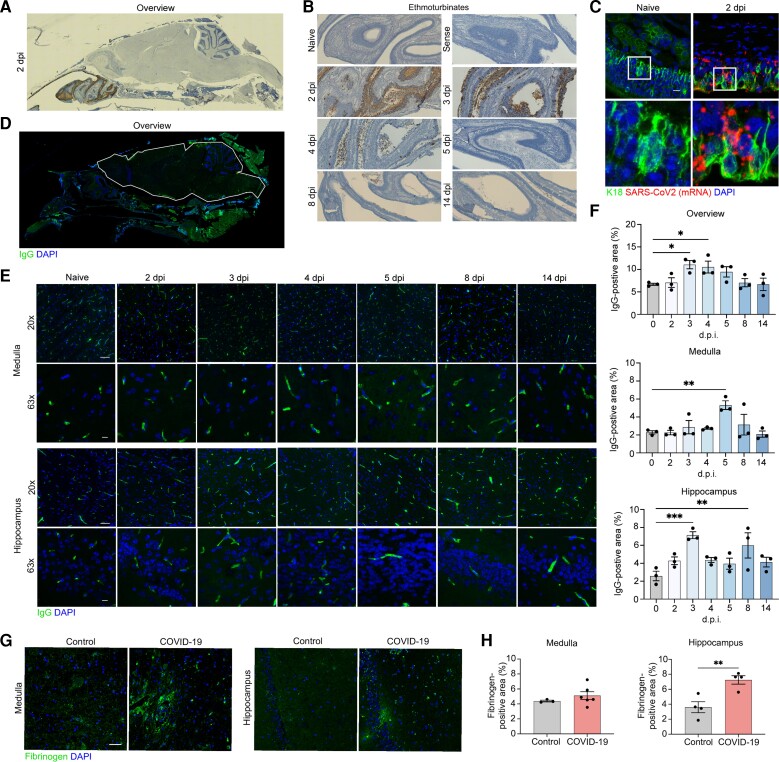
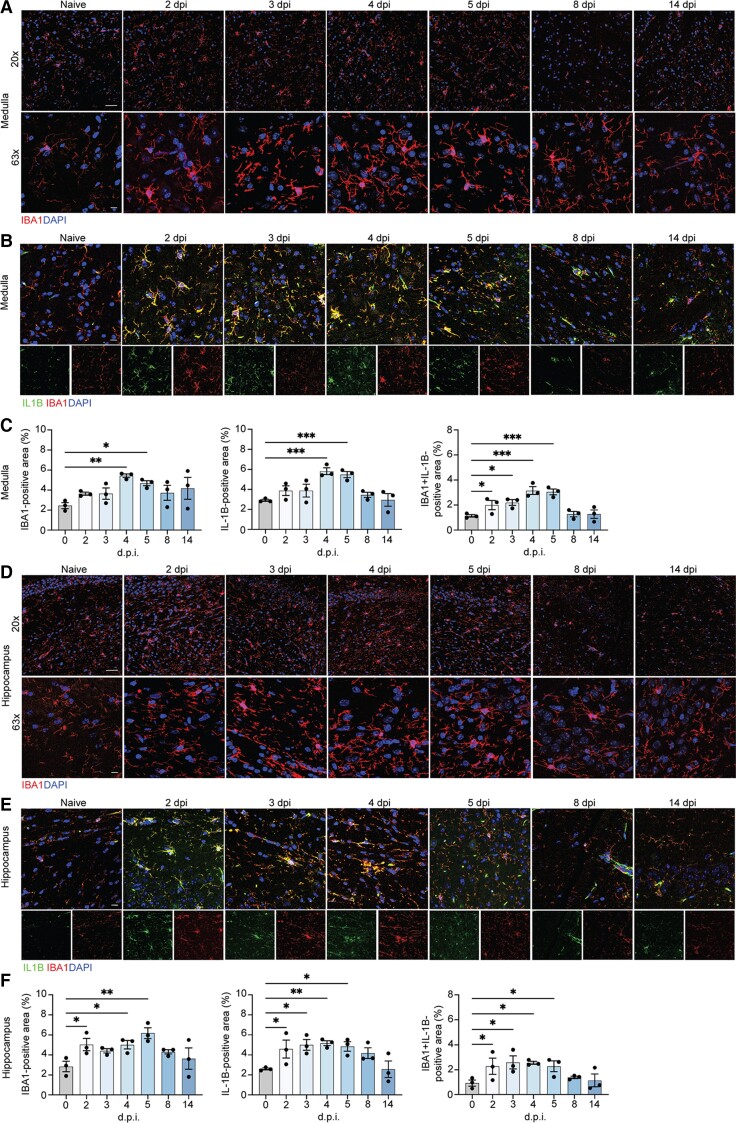
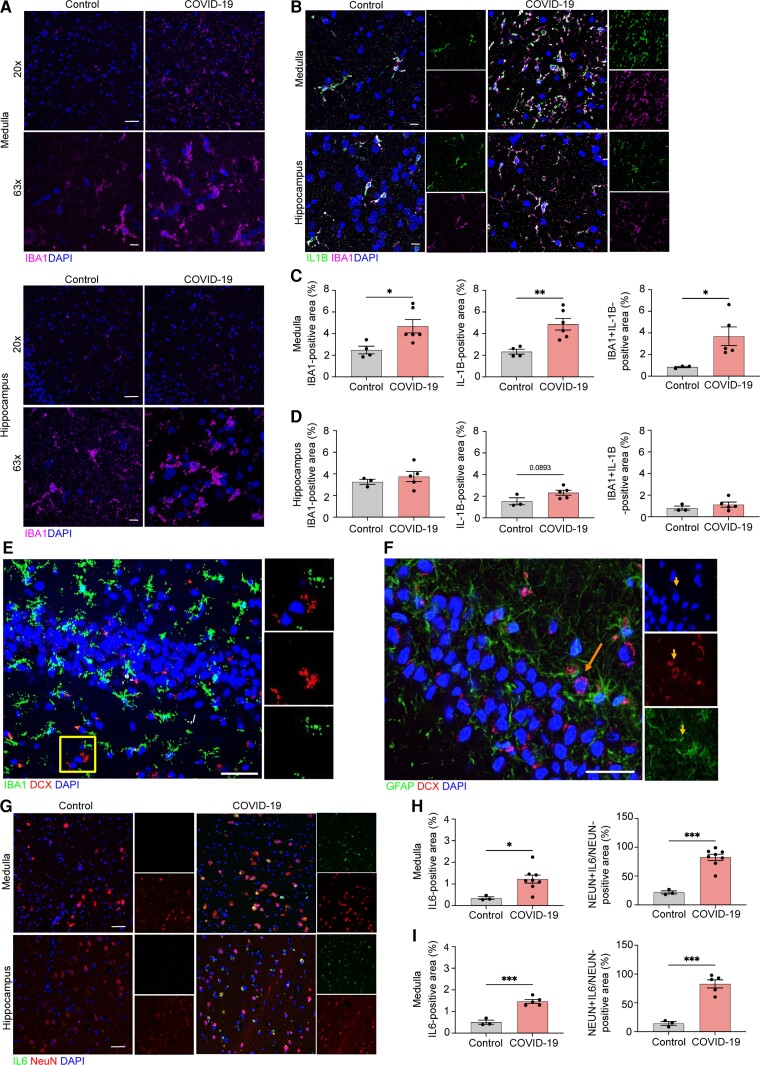
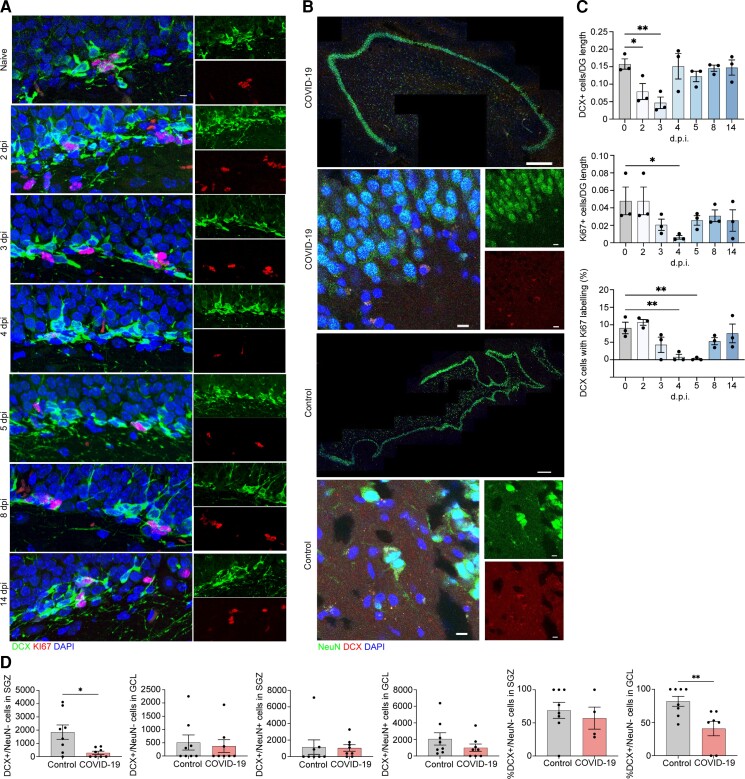
Infection with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is associated with acute and postacute cognitive and neuropsychiatric symptoms including impaired memory, concentration, attention, sleep and affect. Mechanisms underlying these brain symptoms remain understudied. Here we report that SARS-CoV-2-infected hamsters exhibit a lack of viral neuroinvasion despite aberrant blood-brain barrier permeability. Hamsters and patients deceased from coronavirus disease 2019 (COVID-19) also exhibit microglial activation and expression of interleukin (IL)-1β and IL-6, especially within the hippocampus and the medulla oblongata, when compared with non-COVID control hamsters and humans who died from other infections, cardiovascular disease, uraemia or trauma. In the hippocampal dentate gyrus of both COVID-19 hamsters and humans, we observed fewer neuroblasts and immature neurons. Protracted inflammation, blood-brain barrier disruption and microglia activation may result in altered neurotransmission, neurogenesis and neuronal damage, explaining neuropsychiatric presentations of COVID-19. The involvement of the hippocampus may explain learning, memory and executive dysfunctions in COVID-19 patients.
Keywords: COVID-19; SARS-CoV-2; brain; cytokine; neurogenesis.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
Update of
-
COVID-19 induces neuroinflammation and loss of hippocampal neurogenesis.Res Sq [Preprint]. 2021 Oct 29:rs.3.rs-1031824. doi: 10.21203/rs.3.rs-1031824/v1. Res Sq. 2021. Update in: Brain. 2022 Dec 19;145(12):4193-4201. doi: 10.1093/brain/awac270. PMID: 34729556 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 MH098786/MH/NIMH NIH HHS/United States
- R21 AI164769/AI/NIAID NIH HHS/United States
- R35 NS122310/NS/NINDS NIH HHS/United States
- R01 MH083862/MH/NIMH NIH HHS/United States
- R01 MH083862/MH/NIMH NIH HHS/United States
- R56 AI147623/AI/NIAID NIH HHS/United States
- R01 MH040210/MH/NIMH NIH HHS/United States
- F32 NS128065/GF/NIH HHS/United States
- R56 AG063372/AG/NIA NIH HHS/United States
- P50 MH090964/MH/NIMH NIH HHS/United States
- R25 MH086466/MH/NIMH NIH HHS/United States
- U01 NS090415/NS/NINDS NIH HHS/United States
- U01 AI151810/AI/NIAID NIH HHS/United States
- R01 MH125030/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
