

Types of intrapartum hypoxia in the newborn at term with metabolic acidemia: A retrospective study
- PMID: 36004701
- PMCID: PMC9812112
- DOI: 10.1111/aogs.14436
Types of intrapartum hypoxia in the newborn at term with metabolic acidemia: A retrospective study
Abstract
Introduction: In the most recent recommendations of the International Federation of Gynecology and Obstetrics (FIGO), a chapter was dedicated to the physiological approach and to the description of fetal mechanisms developed to respond to hypoxia. Our objective was to classify the type of hypoxia in the case of metabolic acidemia and to describe the order of appearance of fetal heart rate abnormalities in cases of gradually evolving hypoxia.
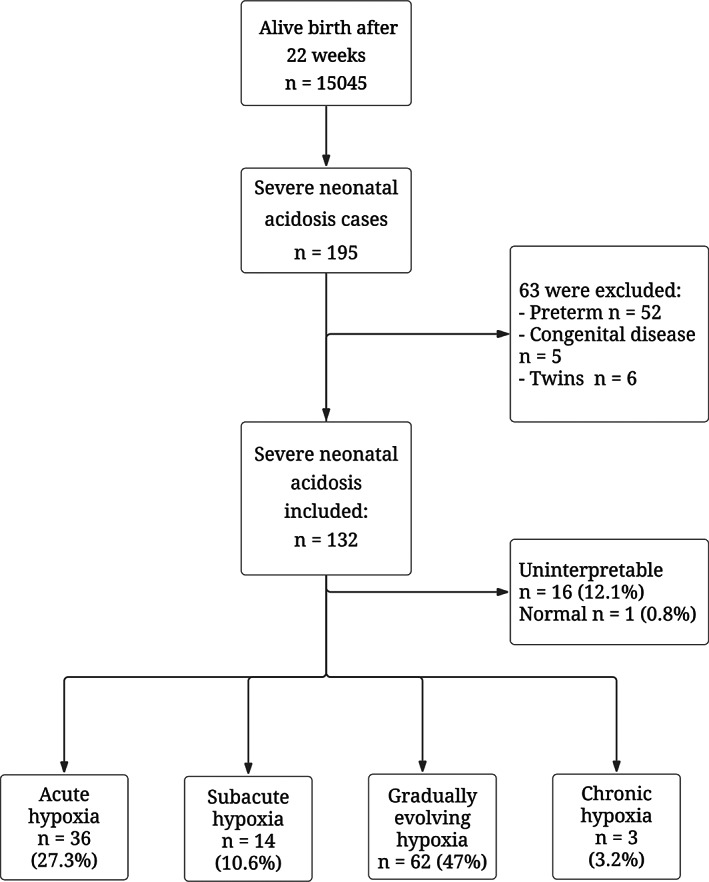
Material and methods: 132 neonates born between 2018 and 2020 with acidemia were included. We excluded preterm birth, fetuses with congenital anomaly and twin pregnancies. Intrapartum cardiotocography traces were assigned to one of these four types of labor hypoxia: acute, subacute, gradually evolving and chronic hypoxia. For gradually evolving hypoxia, fetal heart rate abnormalities were described according to the FIGO classification.
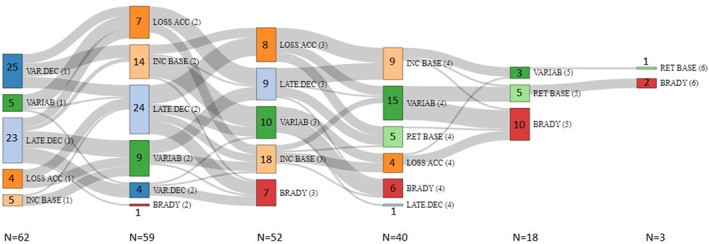
Results: 36 cardiotocography traces (27.3%) were classified as acute hypoxia, 14 (10.6%) as subacute hypoxia, and 3 (3.2%) as chronic hypoxia; gradually evolving hypoxia occurred in 62 cases (47%). In 77.4% of cases of gradually evolving hypoxia, deceleration was the first anomaly to appear, with loss of variability and bradycardia appearing later. Increased fetal heart rate was observed immediately after late deceleration in 46.8% of cases and was followed by a loss of variability or saltatory rhythm in 37.1% of cases.
Conclusions: In cases of metabolic acidemia at term, the most frequent situation observed was gradually evolving hypoxia, with an initial occurrence of decelerations. The sequence of fetal heart rate modifications was variable.
Keywords: chemoreflex; deceleration; fetal heart rate; hypoxia; intrapartum CTG; neonatal acidemia; variability.
© 2022 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
None declared.
Figures
Similar articles
-
Quantification of Posterior Risk Related to Intrapartum FIGO 2015 Criteria for Cardiotocography in the Second Stage of Labor.Fetal Diagn Ther. 2021;48(2):149-157. doi: 10.1159/000512658. Epub 2021 Jan 28. Fetal Diagn Ther. 2021. PMID: 33508830
-
Correlation between umbilical vein-to-artery delta pH and type of intrapartum hypoxia in a cohort of acidemic neonates: A retrospective analysis of CTG findings.Eur J Obstet Gynecol Reprod Biol. 2018 Dec;231:25-29. doi: 10.1016/j.ejogrb.2018.10.005. Epub 2018 Oct 3. Eur J Obstet Gynecol Reprod Biol. 2018. PMID: 30317141
-
Impaired validity of the new FIGO and Swedish CTG classification templates to identify fetal acidosis in the first stage of labor.J Matern Fetal Neonatal Med. 2022 Dec;35(25):4853-4860. doi: 10.1080/14767058.2020.1869931. Epub 2021 Jan 6. J Matern Fetal Neonatal Med. 2022. PMID: 33406946
-
Optimizing the management of acute, prolonged decelerations and fetal bradycardia based on the understanding of fetal pathophysiology.Am J Obstet Gynecol. 2023 Jun;228(6):645-656. doi: 10.1016/j.ajog.2022.05.014. Am J Obstet Gynecol. 2023. PMID: 37270260 Review.
-
Pathophysiological interpretation of fetal heart rate tracings in clinical practice.Am J Obstet Gynecol. 2023 Jun;228(6):622-644. doi: 10.1016/j.ajog.2022.05.023. Am J Obstet Gynecol. 2023. PMID: 37270259 Review.
Cited by
-
Increased heart rate variability during evolving fetal hypoxia: Be careful during pushing efforts.Acta Obstet Gynecol Scand. 2024 Mar;103(3):623. doi: 10.1111/aogs.14788. Epub 2024 Jan 24. Acta Obstet Gynecol Scand. 2024. PMID: 38265179 Free PMC article. No abstract available.
-
Suppressed or increased fetal heart rate variability: Which is more associated with intrapartum fetal compromise?Acta Obstet Gynecol Scand. 2024 Mar;103(3):621-622. doi: 10.1111/aogs.14762. Epub 2023 Dec 29. Acta Obstet Gynecol Scand. 2024. PMID: 38158625 Free PMC article. No abstract available.
-
Relative uteroplacental insufficiency of labor.Acta Obstet Gynecol Scand. 2024 Oct;103(10):1910-1918. doi: 10.1111/aogs.14937. Epub 2024 Aug 6. Acta Obstet Gynecol Scand. 2024. PMID: 39107951 Free PMC article. Review.
References
-
- Collége National des Gynécologues et Obstétriciens Français . Modalités de surveillance foetale pendant le travail. Texte des recommandations. [Methods of fetal surveillance during labor. Guidelines]. In French. J Gynecol Obstet Biol Reprod (Paris). 2008;37(suppl 1):S101‐S107. - PubMed
-
- Rhöse S, Heinis AMF, Vandenbussche F, van Drongelen J, van Dillen J. Inter‐ and intra‐observer agreement of non‐reassuring cardiotocography analysis and subsequent clinical management. Acta Obstet Gynecol Scand. 2014;93:596‐602. - PubMed
-
- Chauhan SP, Klauser CK, Woodring TC, Sanderson M, Magann EF, Morrison JC. Intrapartum nonreassuring fetal heart rate tracing and prediction of adverse outcomes: interobserver variability. Am J Obstet Gynecol. 2008;199:623.e1‐623.e5. - PubMed
-
- Alfirevic Z, Devane D, Gyte GML. Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour. Cochrane Database Syst Rev. 2013;5:CD006066. - PubMed
-
- Clark SL, Hamilton EF, Garite TJ, Timmins A, Warrick PA, Smith S. The limits of electronic fetal heart rate monitoring in the prevention of neonatal metabolic acidemia. Am J Obstet Gynecol. 2017;216:163.e1‐163.e6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
