

Pregnancy Considerations in the Multidisciplinary Care of Patients with Pulmonary Arterial Hypertension
- PMID: 36005424
- PMCID: PMC9409449
- DOI: 10.3390/jcdd9080260
Pregnancy Considerations in the Multidisciplinary Care of Patients with Pulmonary Arterial Hypertension
Abstract
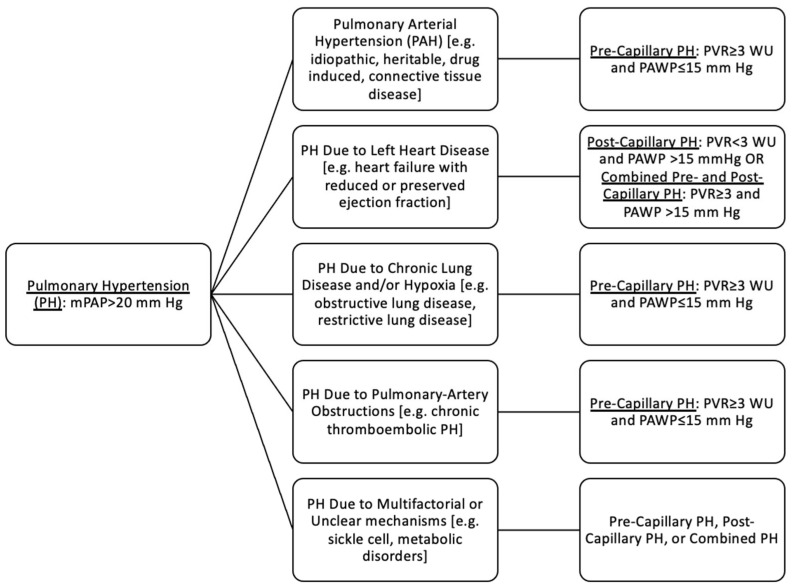
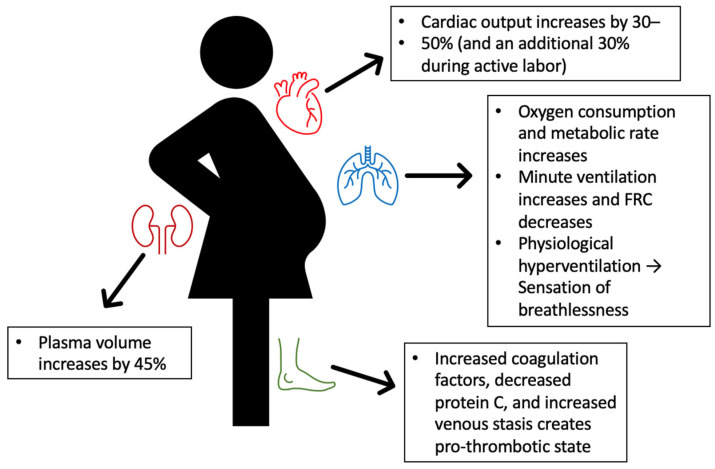
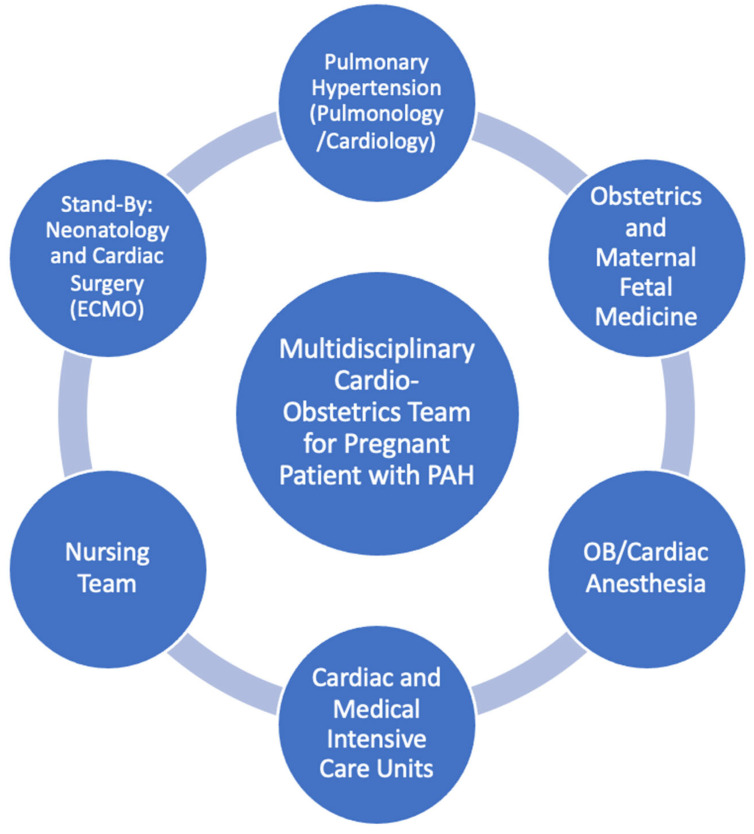
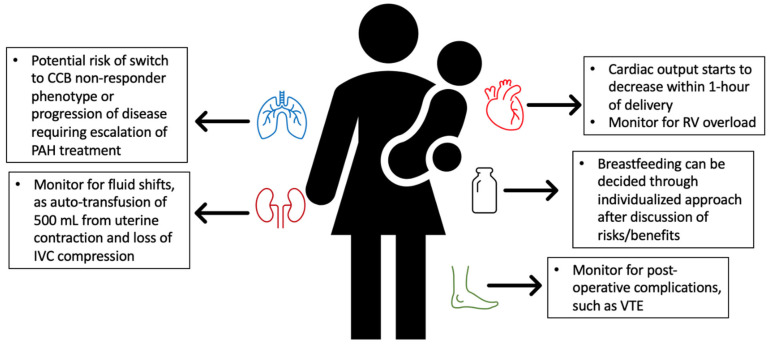
Pulmonary arterial hypertension (PAH) is a vasoconstrictive disease of the distal pulmonary vasculature resulting in adverse right heart remodeling. Pregnancy in PAH patients is associated with high maternal morbidity and mortality as well as neonatal and fetal complications. Pregnancy-associated changes in the cardiovascular, pulmonary, hormonal, and thrombotic systems challenge the complex PAH physiology. Due to the high risks, patients with PAH are currently counseled against pregnancy based on international consensus guidelines, but there are promising signs of improving outcomes, particularly for patients with mild disease. For patients who become pregnant, multidisciplinary care at a PAH specialist center is needed for peripartum monitoring, medication management, delivery, postpartum care, and complication management. Patients with PAH also require disease-specific counseling on contraception and breastfeeding. In this review, we detail the considerations for reproductive planning, pregnancy, and delivery for the multidisciplinary care of a patient with PAH.
Keywords: cardio-obstetrics; peripartum cardiovascular disease; pregnancy; pulmonary hypertension.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Management of pulmonary arterial hypertension during pregnancy.Expert Rev Respir Med. 2023 May;17(5):413-423. doi: 10.1080/17476348.2023.2210838. Epub 2023 May 9. Expert Rev Respir Med. 2023. PMID: 37159412 Review.
-
Pregnancy in Congenital Heart Disease, Complicated by Pulmonary Arterial Hypertension-A Challenging Issue for the Pregnant Woman, the Foetus, and Healthcare Professionals.Medicina (Kaunas). 2022 Mar 25;58(4):476. doi: 10.3390/medicina58040476. Medicina (Kaunas). 2022. PMID: 35454315 Free PMC article.
-
Peripartum outcomes in a large population of women with pulmonary arterial hypertension associated with congenital heart disease.Eur J Prev Cardiol. 2019 Jul;26(10):1067-1076. doi: 10.1177/2047487318821246. Epub 2019 Apr 11. Eur J Prev Cardiol. 2019. PMID: 30971116
-
Management of pulmonary arterial hypertension:before, during and after pregnancy.Int J Cardiol Cardiovasc Risk Prev. 2024 Mar 17;21:200252. doi: 10.1016/j.ijcrp.2024.200252. eCollection 2024 Jun. Int J Cardiol Cardiovasc Risk Prev. 2024. PMID: 38549736 Free PMC article. Review.
-
Perioperative Management of Pregnant Women With Idiopathic Pulmonary Arterial Hypertension: An Observational Case Series Study From China.J Cardiothorac Vasc Anesth. 2018 Dec;32(6):2547-2559. doi: 10.1053/j.jvca.2018.01.043. Epub 2018 Mar 7. J Cardiothorac Vasc Anesth. 2018. PMID: 29525197
Cited by
-
When pulmonary arterial hypertension and pregnancy meet: a multidisciplinary clinical experts review.Arch Gynecol Obstet. 2024 Dec;310(6):2839-2852. doi: 10.1007/s00404-024-07827-1. Epub 2024 Nov 21. Arch Gynecol Obstet. 2024. PMID: 39570387 Review.
-
Clinical outcomes of pregnancy in patients with pulmonary hypertension: A single center observational study.J Cardiothorac Surg. 2025 Apr 16;20(1):199. doi: 10.1186/s13019-025-03435-5. J Cardiothorac Surg. 2025. PMID: 40241218 Free PMC article.
-
A nomogram model for predicting maternal cardiovascular complications and neonatal adverse outcomes in pregnant patients with pulmonary arterial hypertension.Ann Med. 2025 Dec;57(1):2541093. doi: 10.1080/07853890.2025.2541093. Epub 2025 Aug 4. Ann Med. 2025. PMID: 40758664 Free PMC article.
-
Exploring the patient perspective in pulmonary hypertension.Eur Respir J. 2024 Oct 31;64(4):2401129. doi: 10.1183/13993003.01129-2024. Print 2024 Oct. Eur Respir J. 2024. PMID: 39209479 Free PMC article.
-
Epoprostenol Exposure During Pregnancy.Crit Care Explor. 2023 Jun 5;5(6):e0928. doi: 10.1097/CCE.0000000000000928. eCollection 2023 Jun. Crit Care Explor. 2023. PMID: 37637356 Free PMC article.
References
-
- Vonk-Noordegraaf A., Haddad F., Chin K.M., Forfia P., Kawut S., Lumens J., Naeije R., Newman J., Oudiz R., Pro-vencher S., et al. Right heart adaptation to pulmonary arterial hypertension: Physiology and pathobiology. J. Am. Coll. Cardiol. 2013;62:D22–D33. doi: 10.1016/j.jacc.2013.10.027. - DOI - PubMed
-
- Vonk-Noordegraaf A., Chin K.M., Haddad F., Hassoun P., Hemnes A., Hopkins S., Kawut S., Langleben D., Lumens J., Naeije R. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: An update. Eur. Respir. J. 2019;53:1801900. doi: 10.1183/13993003.01900-2018. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
