

At the Crossroads of Minimally Invasive Mitral Valve Surgery-Benching Single Hospital Experience to a National Registry: A Plea for Risk Management Technology
- PMID: 36005425
- PMCID: PMC9410306
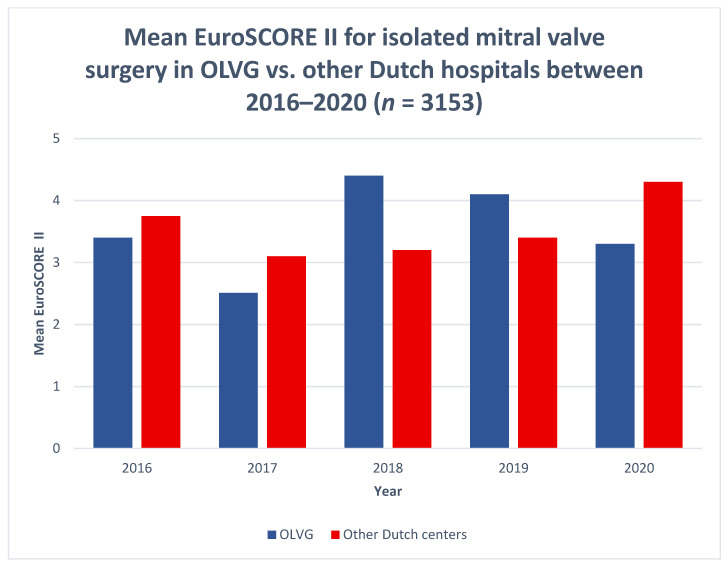
- DOI: 10.3390/jcdd9080261
At the Crossroads of Minimally Invasive Mitral Valve Surgery-Benching Single Hospital Experience to a National Registry: A Plea for Risk Management Technology
Abstract
Almost 30 years after the first endoscopic mitral valve repair, Minimally Invasive Mitral Valve Surgery (MIMVS) has become the standard at many institutions due to optimal clinical results and fast recovery. The question that arises is can already good results be further improved by an Institutional Risk Management Performance (IRMP) system in decreasing risks in minimally invasive mitral valve surgery (MIMVS)? As of yet, there are no reports on IRMP and learning systems in the literature. (2) Methods: We described and appraised our five-year single institutional experience with MIMVS in isolated valve surgery included in the Netherlands Heart Registry (NHR) and investigated root causes of high-impact complications. (3) Results: The 120-day and 12-month mortality were 1.1% and 1.9%, respectively, compared to the average of 4.3% and 5.3% reported in the NHR. The regurgitation rate was 1.4% compared to 5.2% nationwide. The few high-impact complications appeared not to be preventable. (4) Discussion: In MIMVS, freedom from major and minor complications is a strong indicator of an effective IRMP but remains concealed from physicians and patients, despite its relevance to shared decision making. Innovation adds to the complexity of MIMVS and challenges surgical competence. An IRMP system may detect and control new risks earlier. (5) Conclusion: An IRMP system contributes to an effective reduction of risks, pain and discomfort; provides relevant input for shared decision making; and warrants the safe introduction of new technology. Crossroads conclusions: investment in machine learning and AI for an effective IRMP system is recommended and the roles for commanding and operating surgeons should be considered.
Keywords: minimally invasive mitral valve surgery; risk management; risk management methods; simulator training; surgical training.
Conflict of interest statement
R.C., R.R. and I.M. are working at the OLVG hospital, where data to support the current study was obtained. The authors declare no further conflict of interest.
Figures
Similar articles
-
The evolution of technical prerequisites and local boundary conditions for optimization of mitral valve interventions-Emphasis on skills development and institutional risk performance.Front Cardiovasc Med. 2023 Jul 21;10:1101337. doi: 10.3389/fcvm.2023.1101337. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37547244 Free PMC article. Review.
-
Effect of minimally invasive mitral valve surgery compared to sternotomy on short- and long-term outcomes: a retrospective multicentre interventional cohort study based on Netherlands Heart Registration.Eur J Cardiothorac Surg. 2022 May 2;61(5):1099-1106. doi: 10.1093/ejcts/ezab507. Eur J Cardiothorac Surg. 2022. PMID: 34878099
-
Cross-sectional survey on minimally invasive mitral valve surgery.Ann Cardiothorac Surg. 2013 Nov;2(6):733-8. doi: 10.3978/j.issn.2225-319X.2013.11.11. Ann Cardiothorac Surg. 2013. PMID: 24349974 Free PMC article.
-
The analysis of left ventricular ejection fraction after minimally invasive surgery for primary mitral valve regurgitation.J Card Surg. 2021 Feb;36(2):661-669. doi: 10.1111/jocs.15256. Epub 2020 Dec 18. J Card Surg. 2021. PMID: 33336536
-
Can we use minimally invasive mitral valve surgery as a safe alternative to sternotomy in high-risk patients?Interact Cardiovasc Thorac Surg. 2016 Jan;22(1):92-6. doi: 10.1093/icvts/ivv275. Epub 2015 Oct 8. Interact Cardiovasc Thorac Surg. 2016. PMID: 26451001 Review.
Cited by
-
The evolution of technical prerequisites and local boundary conditions for optimization of mitral valve interventions-Emphasis on skills development and institutional risk performance.Front Cardiovasc Med. 2023 Jul 21;10:1101337. doi: 10.3389/fcvm.2023.1101337. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37547244 Free PMC article. Review.
-
Elderly patients benefit from minimally invasive mitral valve surgery: perioperative risk management matters.Interdiscip Cardiovasc Thorac Surg. 2024 Jan 2;38(1):ivad211. doi: 10.1093/icvts/ivad211. Interdiscip Cardiovasc Thorac Surg. 2024. PMID: 38191999 Free PMC article.
References
-
- Zegers M., De Bruijne M.C., De Keizer B., Merten H., Groenewegen P.P., Van Der Wal G., Wagner C. The incidence, root-causes, and outcomes of adverse events in surgical units: Implication for potential prevention strategies. Patient Saf. Surg. 2011;5:13. doi: 10.1186/1754-9493-5-13. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
