

Overcoming High Impedance in the Transitional Area of the Distal Great Cardiac Vein during Radiofrequency Catheter Ablation of Ventricular Arrhythmia
- PMID: 36005428
- PMCID: PMC9410161
- DOI: 10.3390/jcdd9080264
Overcoming High Impedance in the Transitional Area of the Distal Great Cardiac Vein during Radiofrequency Catheter Ablation of Ventricular Arrhythmia
Abstract
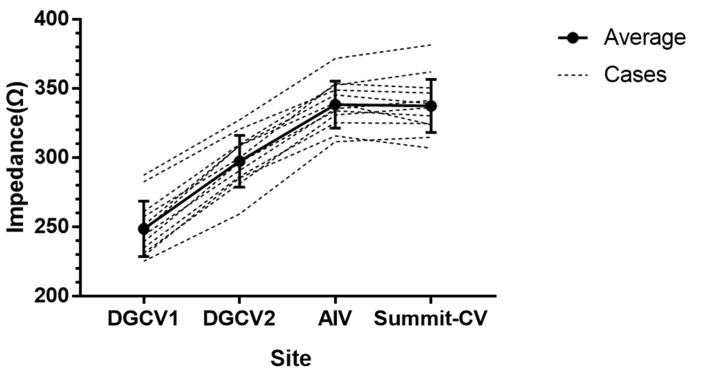
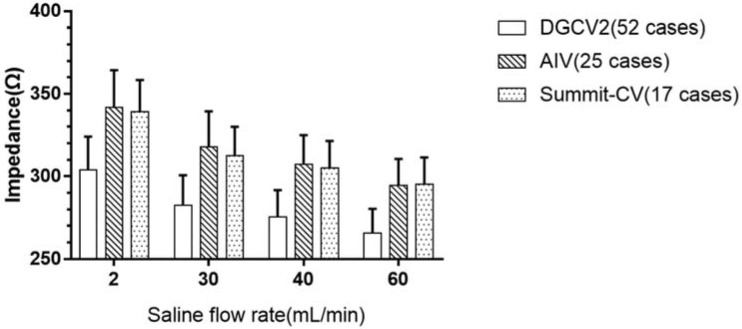
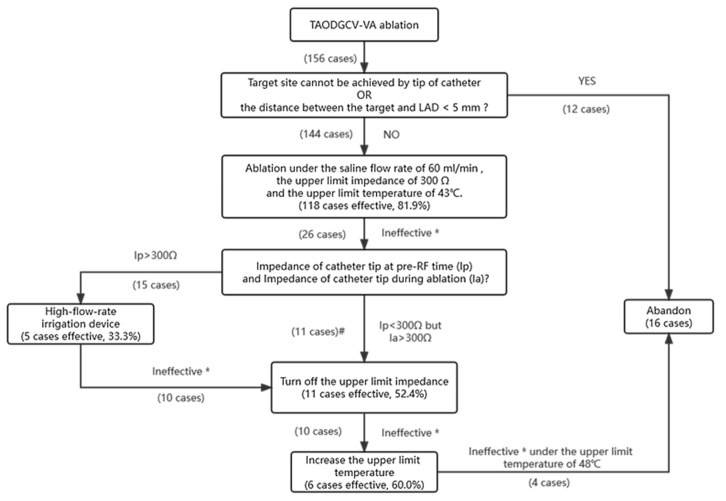
(1) Background: Radiofrequency catheter ablation (RFCA) is an essential treatment for ventricular arrhythmia (VA). However, high impedance in the transitional area of the distal great cardiac vein (TAODGCV) often leads to ablation failure. This study aimed to explore the factors influencing impedance and identify effective ways to reduce impedance. (2) Methods: A total of 156 patients with VA arising from the TAODGCV received RFCA therapy at our center from October 2009 to August 2021 and were retrospectively analyzed. Local impedance variation during RFCA was monitored, recorded, and analyzed. (3) Results: The impedance increased from the proximal to distal portions of the TAODGCV and decreased by increasing the saline flow rate at the same site. To overcome high impedance, we implemented the following strategies: (1) Reset the upper limit impedance to 300 Ω and accelerate the saline flow rate to 60 mL/min (effective in 118 of 144 patients); (2) turn off the upper limit impedance (effective in eleven of 21 patients); (3) use high-flow-rate irrigation devices (effective in five of 15 patients); and (4) increase the upper limit temperature (effective in six of ten patients). (4) Conclusions: In the TAODGCV, local impedance is mainly influenced by the target site location and saline flow rate. We concluded several methods to overcome the high impedance and contribute to a successful ablation.
Keywords: Impedance; distal great cardiac vein; electrophysiology; radiofrequency catheter ablation; ventricular arrhythmia.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
Idiopathic premature ventricular complexes originating from the distal great cardiac vein: Clinical, cardiac and electrophysiological characteristics and catheter ablation outcome.Life Sci. 2018 Jun 1;202:61-69. doi: 10.1016/j.lfs.2018.04.001. Epub 2018 Apr 4. Life Sci. 2018. PMID: 29625195
-
Catheter ablation of idiopathic ventricular arrhythmias originating from left ventricular epicardium adjacent to the transitional area from the great cardiac vein to the anterior interventricular vein.Int J Cardiol. 2013 Sep 10;167(6):2673-81. doi: 10.1016/j.ijcard.2012.06.119. Epub 2012 Jul 16. Int J Cardiol. 2013. PMID: 22805549
-
[Radiofrequency catheter ablation in the treatment of arrhythmias in children--efficacy, safety of the method, predictors of the procedural course and acute success].Przegl Lek. 2009;66(8):418-23. Przegl Lek. 2009. PMID: 20043588 Polish.
-
Modulating the Baseline Impedance: An Adjunctive Technique for Maximizing Radiofrequency Lesion Dimensions in Deep and Intramural Ventricular Substrate: An Adjunctive Technique for Maximizing Radiofrequency Lesion Dimensions in Deep and Intramural Ventricular Substrate.Circ Arrhythm Electrophysiol. 2019 Jun;12(6):e007336. doi: 10.1161/CIRCEP.119.007336. Circ Arrhythm Electrophysiol. 2019. PMID: 31113232 Free PMC article.
-
Approach selection of radiofrequency catheter ablation for ventricular arrhythmias originating from the left ventricular summit: potential relevance of Pseudo Delta wave, Intrinsicoid deflection time, maximal deflection index.BMC Cardiovasc Disord. 2017 May 30;17(1):140. doi: 10.1186/s12872-017-0575-5. BMC Cardiovasc Disord. 2017. PMID: 28558750 Free PMC article.
Cited by
-
Ventricular arrhythmias originating from different portions of the communicating vein of the left ventricular summit: electrocardiographic characteristics and catheter ablation.BMC Cardiovasc Disord. 2024 Aug 13;24(1):421. doi: 10.1186/s12872-024-04099-0. BMC Cardiovasc Disord. 2024. PMID: 39134935 Free PMC article.
References
-
- Zhu D.W.X., Maloney J.D., Simmons T.W., Nitta J., Fitzgerald D.M., Trohman R.G., Khoury D.S., Saliba W., Belco K.M., Rizo-Patron C., et al. Radiofrequency catheter ablation for management of symptomatic ventricular ectopic activity. J. Am. Coll. Cardiol. 1995;26:843–849. doi: 10.1016/0735-1097(95)00287-7. - DOI - PubMed
-
- Bogun F., Crawford T., Reich S., Koelling T.M., Armstrong W., Good E., Jongnarangsin K., Marine J.E., Chugh A., Pelosi F., et al. Radiofrequency ablation of frequent, idiopathic premature ventricular complexes: Comparison with a control group without intervention. Heart Rhythm. 2007;4:863–867. doi: 10.1016/j.hrthm.2007.03.003. - DOI - PubMed
-
- Takemoto M., Yoshimura H., Ohba Y., Matsumoto Y., Yamamoto U., Mohri M., Yamamoto H., Origuchi H. Radiofrequency Catheter Ablation of Premature Ventricular Complexes From Right Ventricular Outflow Tract Improves Left Ventricular Dilation and Clinical Status in Patients Without Structural Heart Disease. J. Am. Coll. Cardiol. 2005;45:1259–1265. doi: 10.1016/j.jacc.2004.12.073. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
