

Cardiac Complications of Hypertensive Emergency: Classification, Diagnosis and Management Challenges
- PMID: 36005440
- PMCID: PMC9409837
- DOI: 10.3390/jcdd9080276
Cardiac Complications of Hypertensive Emergency: Classification, Diagnosis and Management Challenges
Abstract
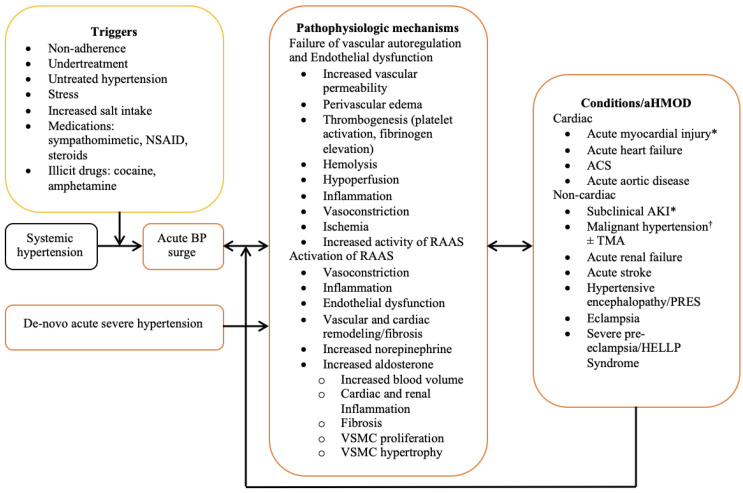
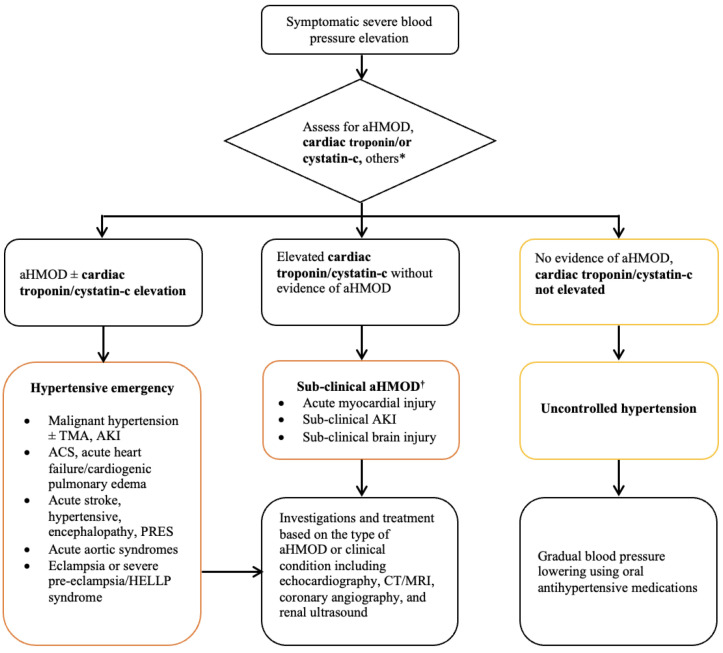
While mortality in patients with hypertensive emergency has significantly improved over the past decades, the incidence and complications associated with acute hypertension-mediated organ damage have not followed a similar trend. Hypertensive emergency is characterized by an abrupt surge in blood pressure, mostly occurring in people with pre-existing hypertension to result in acute hypertension-mediated organ damage. Acute hypertension-mediated organ damage commonly affects the cardiovascular system, and present as acute heart failure, myocardial infarction, and less commonly, acute aortic syndrome. Elevated cardiac troponin with or without myocardial infarction is one of the major determinants of outcome in hypertensive emergency. Despite being an established entity distinct from myocardial infarction, myocardial injury has not been systematically studied in hypertensive emergency. The current guidelines on the evaluation and management of hypertensive emergencies limit the cardiac troponin assay to patients presenting with features of myocardial ischemia and acute coronary syndrome, resulting in underdiagnosis, especially of atypical myocardial infarction. In this narrative review, we aimed to give an overview of the epidemiology and pathophysiology of hypertensive emergencies, highlight challenges in the evaluation, classification, and treatment of hypertensive emergency, and propose an algorithm for the evaluation and classification of cardiac acute hypertension-mediated organ damage.
Keywords: cardiac acute hypertension-mediated organ damage; classifications; diagnosis; epidemiology; hypertensive emergency; myocardial injury; pathophysiology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Clinical Outcomes in Hypertensive Emergency: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2023 Jul 18;12(14):e029355. doi: 10.1161/JAHA.122.029355. Epub 2023 Jul 8. J Am Heart Assoc. 2023. PMID: 37421281 Free PMC article.
-
[Hypertensive emergency and urgence].Herz. 2003 Dec;28(8):717-24. doi: 10.1007/s00059-003-2506-8. Herz. 2003. PMID: 14689106 Review. German.
-
Clinical Profile of Patients with Hypertensive Emergency Referred to a Tertiary Hospital in the Western Cape Province of South Africa.Curr Hypertens Rev. 2023;19(3):194-205. doi: 10.2174/0115734021266958231101094556. Curr Hypertens Rev. 2023. PMID: 37957866
-
Trends in Hospitalization for Hypertensive Emergency, and Relationship of End-Organ Damage With In-Hospital Mortality.Am J Hypertens. 2017 Jul 1;30(7):700-706. doi: 10.1093/ajh/hpx048. Am J Hypertens. 2017. PMID: 28430850
-
[Cardiovascular complications of hypertensive crisis].Rev Med Inst Mex Seguro Soc. 2016;54 Suppl 1:s67-74. Rev Med Inst Mex Seguro Soc. 2016. PMID: 27284845 Review. Spanish.
Cited by
-
Slow on the Draw-ED Management of Elevated BP in Older Adults.Curr Hypertens Rep. 2024 Mar;26(3):107-117. doi: 10.1007/s11906-023-01284-y. Epub 2023 Nov 21. Curr Hypertens Rep. 2024. PMID: 37987967 Review.
-
Value of internet of things-based diagnosis-treatment model in improving the quality of medical services during COVID-19 outbreak.Am J Transl Res. 2023 Jan 15;15(1):573-581. eCollection 2023. Am J Transl Res. 2023. PMID: 36777865 Free PMC article.
-
Metalloproteinases (MMPs) in hypertensive disorders: role, function, pharmacology, and potential strategies to mitigate pathophysiological changes.Front Pharmacol. 2025 May 26;16:1559288. doi: 10.3389/fphar.2025.1559288. eCollection 2025. Front Pharmacol. 2025. PMID: 40492135 Free PMC article. Review.
-
Can Cardiometabolic Risk Be Reduced in the Elderly? Comprehensive Epidemiological Study.Geriatrics (Basel). 2023 Jul 1;8(4):73. doi: 10.3390/geriatrics8040073. Geriatrics (Basel). 2023. PMID: 37489321 Free PMC article.
-
Robust Estimation of Unsteady Beat-to-Beat Systolic Blood Pressure Trends Using Photoplethysmography Contextual Cycles.Sensors (Basel). 2025 Jun 9;25(12):3625. doi: 10.3390/s25123625. Sensors (Basel). 2025. PMID: 40573512 Free PMC article.
References
-
- van den Born B.-J.H., Lip G.Y., Brguljan-Hitij J., Cremer A., Segura J., Morales E., Mahfoud F., Amraoui F., Persu A., Kahan T., et al. ESC Council on hypertension position document on the management of hypertensive emergencies. Eur. Heart J. Cardiovasc. Pharmacother. 2019;5:37–46. doi: 10.1093/ehjcvp/pvy032. - DOI - PubMed
-
- Mishima E., Funayama Y., Suzuki T., Mishima F., Nitta F., Toyohara T., Kikuchi K., Kunikata H., Hashimoto J., Miyazaki M., et al. Concurrent analogous organ damage in the brain, eyes, and kidneys in malignant hypertension: Reversible encephalopathy, serous retinal detachment, and proteinuria. Hypertens. Res. 2021;44:88–97. doi: 10.1038/s41440-020-0521-2. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
