

Partial Anomalous Left Pulmonary Artery Anterior Versus Posterior Types: A Systematic Review
- PMID: 36006061
- PMCID: PMC9416361
- DOI: 10.3390/tomography8040163
Partial Anomalous Left Pulmonary Artery Anterior Versus Posterior Types: A Systematic Review
Abstract
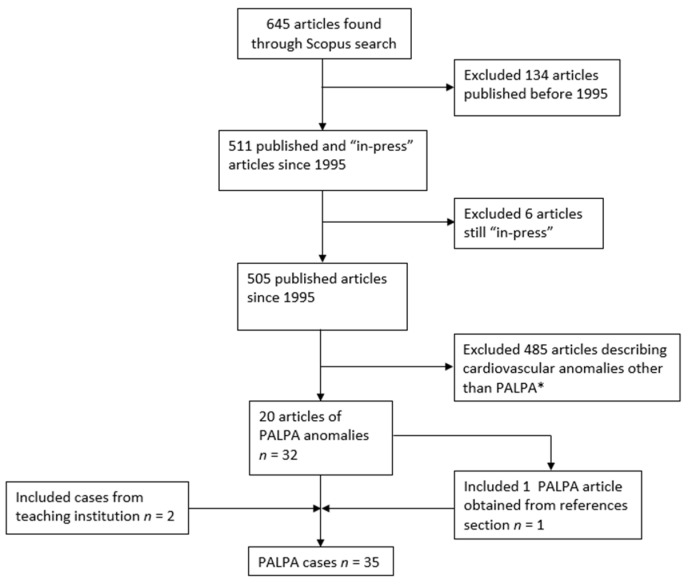
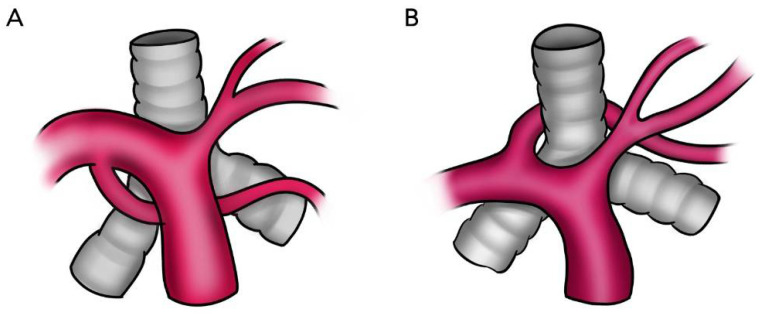
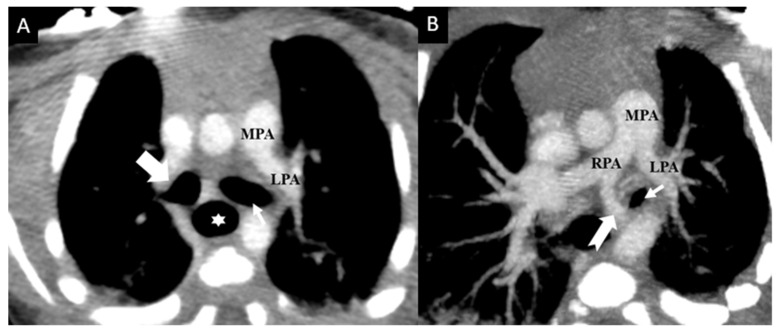
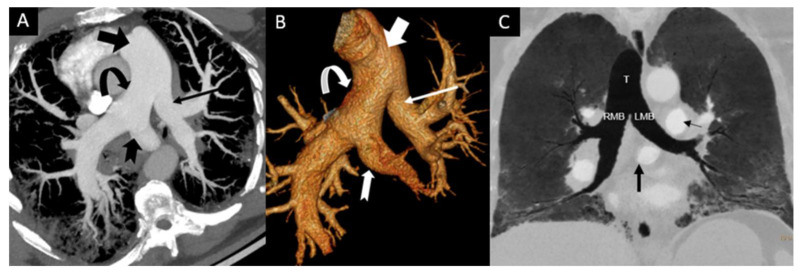
The aim of this study was to investigate the features of partial anomalous left pulmonary artery (PALPA) and differences between cases with posterior versus anterior a nomalous vessels in relation to the tracheobronchial tree. We hypothesized that statistical significance was dependent on the course of the anomalous vessel due to airway compression in the posterior type. This study included cases obtained from the literature (n = 33) and an institution teaching file (n = 2). Information collected: age, sex, medical history, additional anomalies, anomalous vessel course, and respiratory symptoms. Data were analyzed with independent samples t-test and Fisher's exact test. PALPAs were more commonly anterior than posterior. Mean age: 5.3 years (SD = 12.4) for anterior and 6.8 years (SD = 18.5) for posterior (p = 0.77). Respiratory symptoms: 20% of anterior and 60% of posterior cases (p = 0.032). Tracheobronchial anomalies: 35% of anterior and 60% of posterior cases (p = 0.182). Non-cardiac and non-tracheobronchial anomalies: 30% of anterior and 47% of posterior cases (p = 0.511). Kabuki syndrome: 25% of anterior and 6.7% of posterior cases (p = 0.207). In conclusion, respiratory symptoms were the only significant difference between anterior and posterior PALPA types.
Keywords: Kabuki syndrome; congenital heart disease; duplicated left pulmonary artery; partial anomalous left pulmonary artery (PALPA); pseudopulmonary artery sling.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Xie J., Juan Y.H., Wang Q., Chen J., Zhuang J., Xie Z., Liang C., Zhu Y., Yu Z., Li J., et al. Evaluation of left pulmonary artery sling, associated cardiovascular anomalies, and surgical outcomes using cardiovascular computed tomography angiography. Sci. Rep. 2017;7:40042. doi: 10.1038/srep40042. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
