

Comparison of pulmonary function changes between patients receiving neoadjuvant chemotherapy and chemoradiotherapy prior to minimally invasive esophagectomy: a randomized and controlled trial
- PMID: 36006505
- PMCID: PMC9640419
- DOI: 10.1007/s00423-022-02646-x
Comparison of pulmonary function changes between patients receiving neoadjuvant chemotherapy and chemoradiotherapy prior to minimally invasive esophagectomy: a randomized and controlled trial
Abstract
Purpose: Adequate pulmonary function is important for patients undergoing surgical resection of esophageal cancer, especially those that received neoadjuvant therapy. However, it is unknown if pre-operative radiation affects pulmonary function differently compared to chemotherapy. The purpose of this study was to compare changes in pulmonary function between patients undergoing minimally invasive esophagectomy (MIE) who received neoadjuvant chemotherapy or chemoradiotherapy.
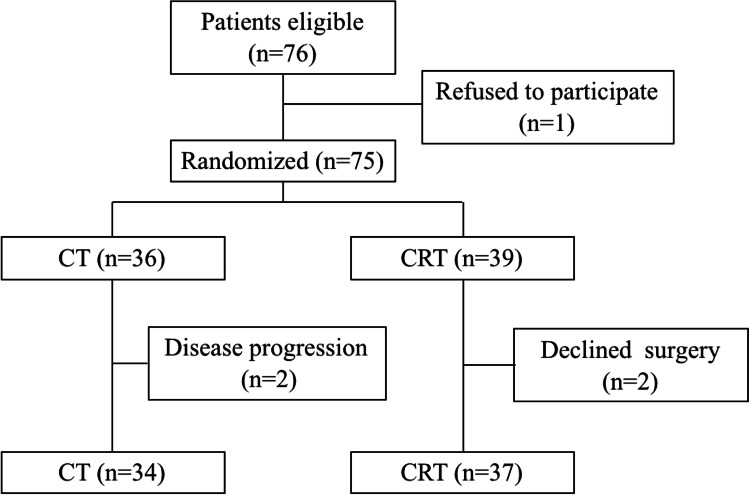
Methods: Between March 2017 and March 2018, esophageal cancer patients requiring neoadjuvant therapy were prospectively enrolled and randomly assigned to receive chemotherapy (CT) or chemoradiotherapy (CRT) before MIE. All patients received pulmonary function testing before and after the neoadjuvant therapy. Changes in pulmonary function, operative data, and pulmonary complications were compared between the 2 groups.
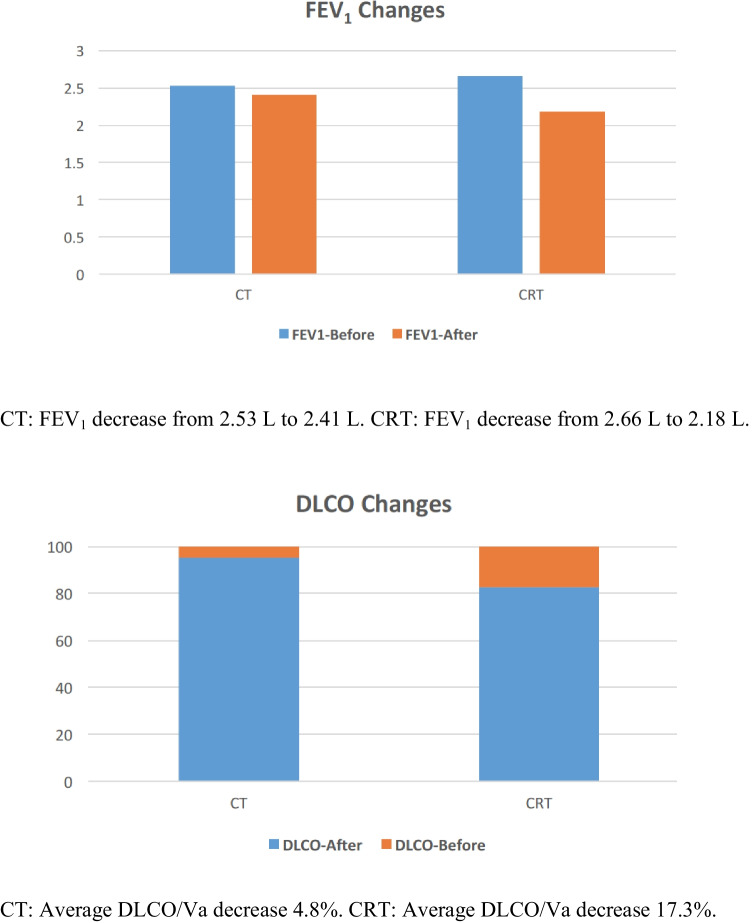
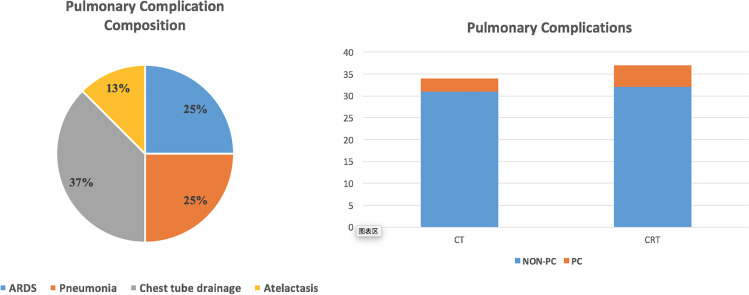
Results: A total of 71 patients were randomized and underwent MIE after receiving CT (n = 34) or CRT (n = 37). Baseline clinical characteristics were comparable between the 2 groups. The CRT group experienced a greater decrease of forced expiratory volume at 1 s (FEV1) (2.66 to 2.18 L, p = 0.023) and diffusion capacity of the lung for carbon monoxide divided by the mean alveolar volume (DLCO/Va) (17.3%, p < 0.001) than the CT group (FEV1 2.53 to 2.41 L; DLCO/Va 4.8%). The incidence of pulmonary complications was higher in the CRT group (13.51 vs. 8.82%), but the difference was not significant (p = 0.532).
Conclusions: Preoperative CRT affects pulmonary function more than CT alone, but does not increase the risk of pulmonary complications in patients undergoing MIE.
Keywords: Esophageal cancer; Neo-adjuvant therapy; Pulmonary function.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Morbidity and Mortality of Patients Who Underwent Minimally Invasive Esophagectomy After Neoadjuvant Chemoradiotherapy vs Neoadjuvant Chemotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: A Randomized Clinical Trial.JAMA Surg. 2021 May 1;156(5):444-451. doi: 10.1001/jamasurg.2021.0133. JAMA Surg. 2021. PMID: 33729467 Free PMC article. Clinical Trial.
-
The impact of tidal volume on pulmonary complications following minimally invasive esophagectomy: a randomized and controlled study.J Thorac Cardiovasc Surg. 2013 Nov;146(5):1267-73; discussion 1273-4. doi: 10.1016/j.jtcvs.2013.06.043. Epub 2013 Aug 28. J Thorac Cardiovasc Surg. 2013. PMID: 23993028 Clinical Trial.
-
CMISG1701: a multicenter prospective randomized phase III clinical trial comparing neoadjuvant chemoradiotherapy to neoadjuvant chemotherapy followed by minimally invasive esophagectomy in patients with locally advanced resectable esophageal squamous cell carcinoma (cT3-4aN0-1M0) (NCT03001596).BMC Cancer. 2017 Jun 28;17(1):450. doi: 10.1186/s12885-017-3446-7. BMC Cancer. 2017. PMID: 28659128 Free PMC article. Clinical Trial.
-
Current Status and Future Prospects for Esophageal Cancer Treatment.Ann Thorac Cardiovasc Surg. 2017 Feb 20;23(1):1-11. doi: 10.5761/atcs.ra.16-00162. Epub 2016 Dec 21. Ann Thorac Cardiovasc Surg. 2017. PMID: 28003586 Free PMC article. Review.
-
Comparison of neoadjuvant chemoradiotherapy and neoadjuvant chemotherapy for esophageal cancer: a meta-analysis.Future Oncol. 2019 Jul;15(20):2413-2422. doi: 10.2217/fon-2019-0024. Epub 2019 Jul 4. Future Oncol. 2019. PMID: 31269806
Cited by
-
Effect of Neoadjuvant Immunotherapy Combined with Chemotherapy on Pulmonary Function and Postoperative Pulmonary Complications in Esophageal Cancer: A Retrospective Study.Curr Cancer Drug Targets. 2024;24(10):1061-1070. doi: 10.2174/0115680096280761231229055929. Curr Cancer Drug Targets. 2024. PMID: 38310460
-
Nomograms to predict tumor regression grade (TRG) and ypTNM staging in patients with locally advanced esophageal cancer receiving neoadjuvant therapy.World J Surg Oncol. 2024 Jul 27;22(1):198. doi: 10.1186/s12957-024-03474-7. World J Surg Oncol. 2024. PMID: 39068445 Free PMC article.
-
Physical fitness predicts post-esophagectomy complications after chemoradiotherapy: a pilot study.BMC Sports Sci Med Rehabil. 2025 Apr 30;17(1):106. doi: 10.1186/s13102-025-01158-7. BMC Sports Sci Med Rehabil. 2025. PMID: 40307840 Free PMC article.
-
Neoadjuvant chemoradiation therapy application in radical esophagectomy surgery: Safety and feasibility: A descriptive study in Vietnam.Medicine (Baltimore). 2025 Jan 31;104(5):e41429. doi: 10.1097/MD.0000000000041429. Medicine (Baltimore). 2025. PMID: 39889158 Free PMC article.
References
-
- Shapiro J, van Lanschot JJB, Hulshof M, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16(9):1090–1098. doi: 10.1016/s1470-2045(15)00040-6. - DOI - PubMed
-
- Ychou M, Boige V, Pignon JP, Conroy T, Bouché O, Lebreton G, et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol. 2011;29(13):1715–1721. doi: 10.1200/jco.2010.33.0597. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
