

Multidisciplinary and standardized management of patients with delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage
- PMID: 36006507
- PMCID: PMC9613736
- DOI: 10.1007/s00701-022-05347-y
Multidisciplinary and standardized management of patients with delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage
Abstract
Background: The appropriate management of delayed cerebral ischemia (DCI) after aneurysmal subarachnoid hemorrhage (aSAH) remains uncertain. We aimed to evaluate the effect of implementing a standardized protocol for detection and management of DCI after aSAH on cerebral infarction and functional outcome.
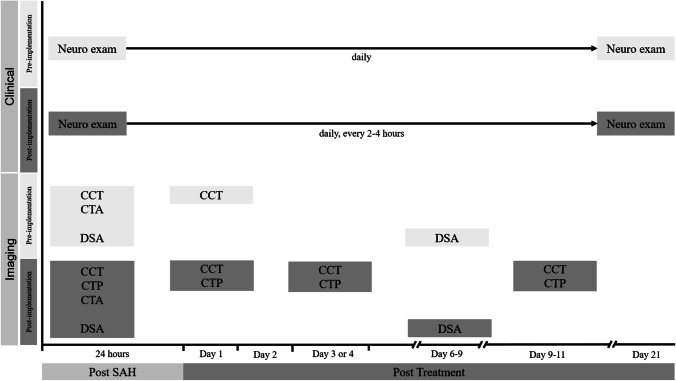
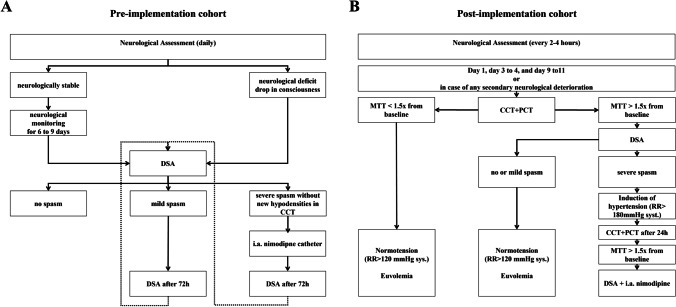
Methods: We studied two cohorts of aSAH patients, one before (pre-implementation cohort: January 2012 to August 2014) and one after (post-implementation cohort: January 2016 to July 2018) implementation of a multidisciplinary approach, with standardized neurological and radiological assessment and risk-based medical treatment of DCI. We assessed the presence of new hypodensities on CT within 6 weeks after aSAH and categorized cerebral infarction into overall and DCI-related infarctions (hypodensities not within 48 h after IA repair and not attributable to aneurysm occlusion or intraparenchymal hematoma). Functional outcome was assessed at 3 months using the extended Glasgow outcome scale (eGOS), dichotomized into unfavorable (eGOS: 1-5) and favorable (eGOS: 6-8). We calculated odds ratios (OR) with corresponding 95% confidence intervals (CI's), and adjusted for age, WFNS grade, Fisher score, and treatment modality (aOR).
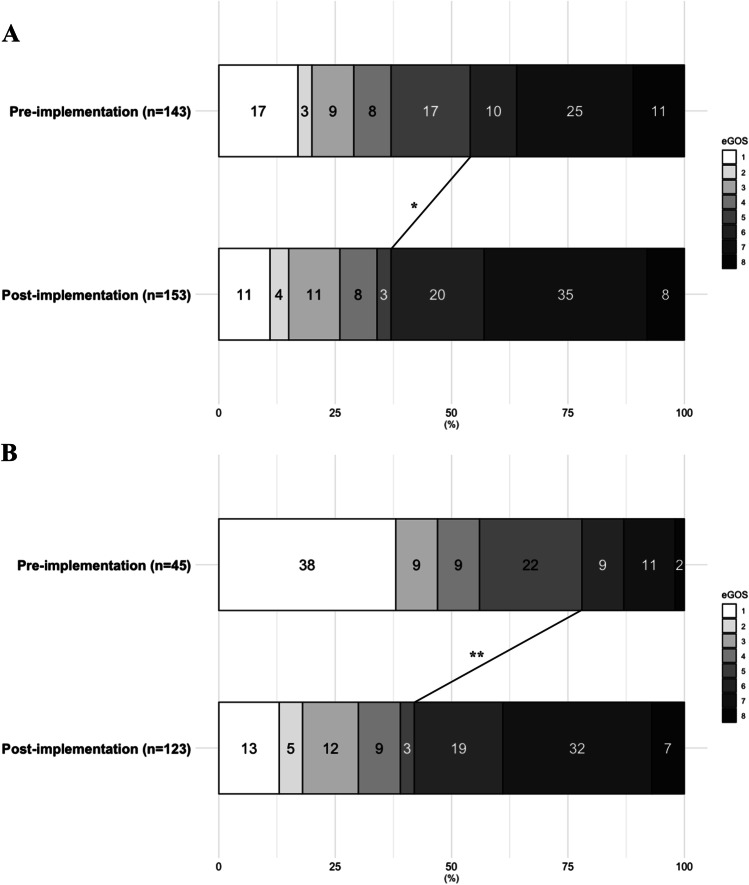
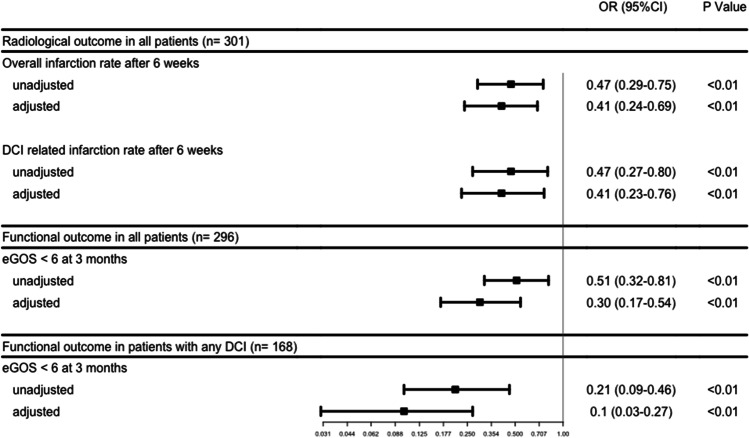
Results: In the post-implementation (n = 158) versus the pre-implementation (n = 143) cohort the rates for overall cerebral infarction were 29.1% vs 46.9% (aOR: 0.41 [0.24-0.69]), for DCI-related cerebral infarction 17.7% vs. 31.5% (aOR: 0.41 [0.23-0.76]), and for unfavorable functional outcome at 3 months 37.3% vs. 53.8% (aOR: 0.30 [0.17-0.54]). For patients with DCI, the rates for unfavorable functional outcomes at 3 months in the post-implementation versus the pre-implementation cohort were 42.3% vs. 77.8% (aOR: 0.1 [0.03-0.27]).
Conclusions: A multidisciplinary approach with more frequent and standardized neurological assessment, standardized CT and CT perfusion monitoring, as well as tailored application of induced hypertension and invasive rescue therapy strategies, is associated with a significant reduction of cerebral infarction and unfavorable functional outcome after aneurysmal aSAH.
Keywords: Delayed cerebral ischemia; Intra-arterial treatment; Perfusion CT; Subarachnoid hemorrhage; Vasospasm.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Adami D, Berkefeld J, Platz J, Konczalla J, Pfeilschifter W, Weidauer S, Wagner M. Complication rate of intraarterial treatment of severe cerebral vasospasm after subarachnoid hemorrhage with nimodipine and percutaneous transluminal balloon angioplasty: worth the risk? J Neuroradiol. 2019;46:15–24. doi: 10.1016/j.neurad.2018.04.001. - DOI - PubMed
-
- Carlson AP, Hanggi D, Wong GK, Etminan N, Mayer SA, Aldrich F, Diringer MN, Schmutzhard E, Faleck HJ, Ng D, Saville BR, Bleck T, Grubb R, Jr, Miller M, Suarez JI, Proskin HM, Macdonald RL, Investigators N. Single-dose intraventricular nimodipine microparticles versus oral nimodipine for aneurysmal subarachnoid hemorrhage. Stroke. 2020;51:1142–1149. doi: 10.1161/STROKEAHA.119.027396. - DOI - PubMed
-
- Cremers CH, van der Schaaf IC, Wensink E, Greving JP, Rinkel GJ, Velthuis BK, Vergouwen MD. CT perfusion and delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. J Cereb Blood Flow Metab. 2014;34:200–207. doi: 10.1038/jcbfm.2013.208. - DOI - PMC - PubMed
-
- Cremers CH, Vos PC, van der Schaaf IC, Velthuis BK, Vergouwen MD, Rinkel GJ, Dankbaar JW. CT perfusion during delayed cerebral ischemia after subarachnoid hemorrhage: distinction between reversible ischemia and ischemia progressing to infarction. Neuroradiology. 2015;57:897–902. doi: 10.1007/s00234-015-1543-3. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
