

Improved joint line and posterior offset restoration in primary total knee replacement using a robotic-assisted surgical technique: An international multi-centre retrospective analysis of matched cohorts
- PMID: 36006969
- PMCID: PMC9409519
- DOI: 10.1371/journal.pone.0272722
Improved joint line and posterior offset restoration in primary total knee replacement using a robotic-assisted surgical technique: An international multi-centre retrospective analysis of matched cohorts
Abstract
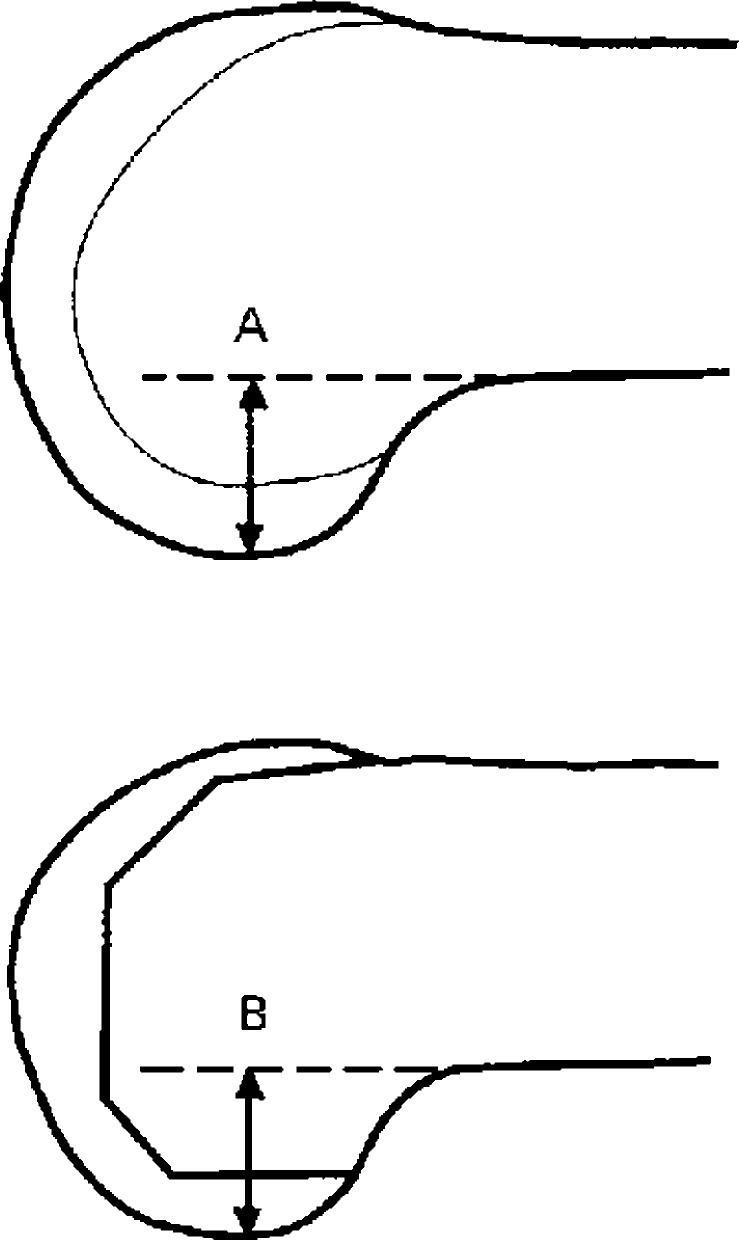
Background: Accurate restoration of joint line height and posterior offset in primary Total Knee Arthroplasty (TKA) have been shown to be important factors in post-operative range of movement and function. The aim of this study was to assess the accuracy of joint line and posterior offset restoration in a group of patients that underwent robotic-assisted TKA (raTKA). A matched cohort of patients that underwent a TKA using a conventional jig-based technique was assessed for comparison. The null hypothesis was that there would be no difference between groups.
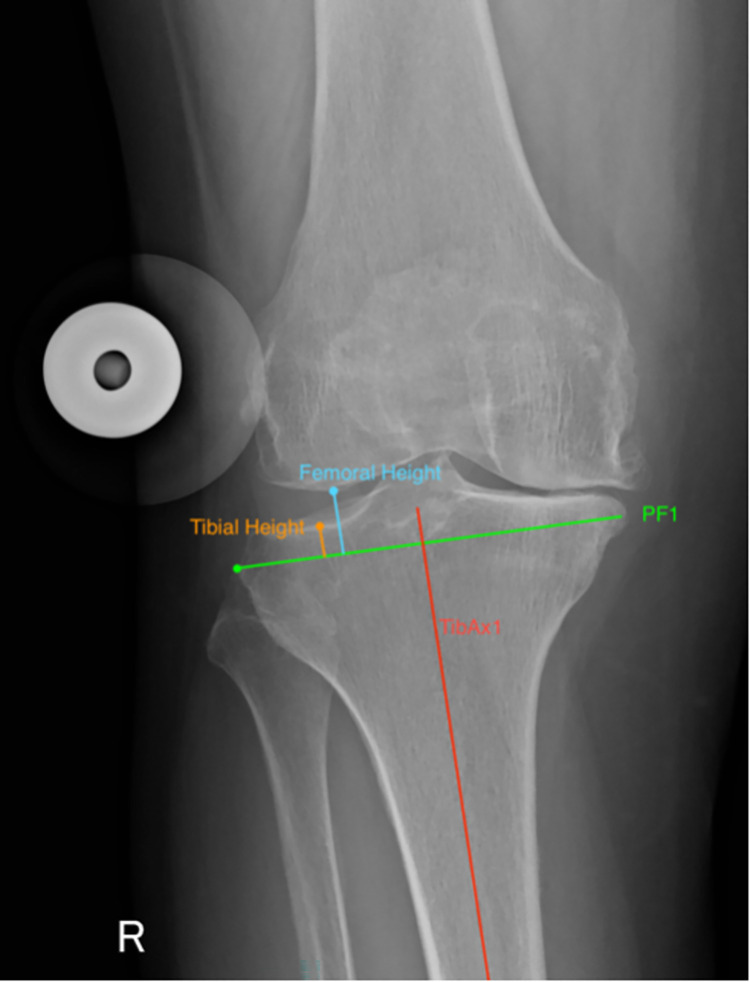
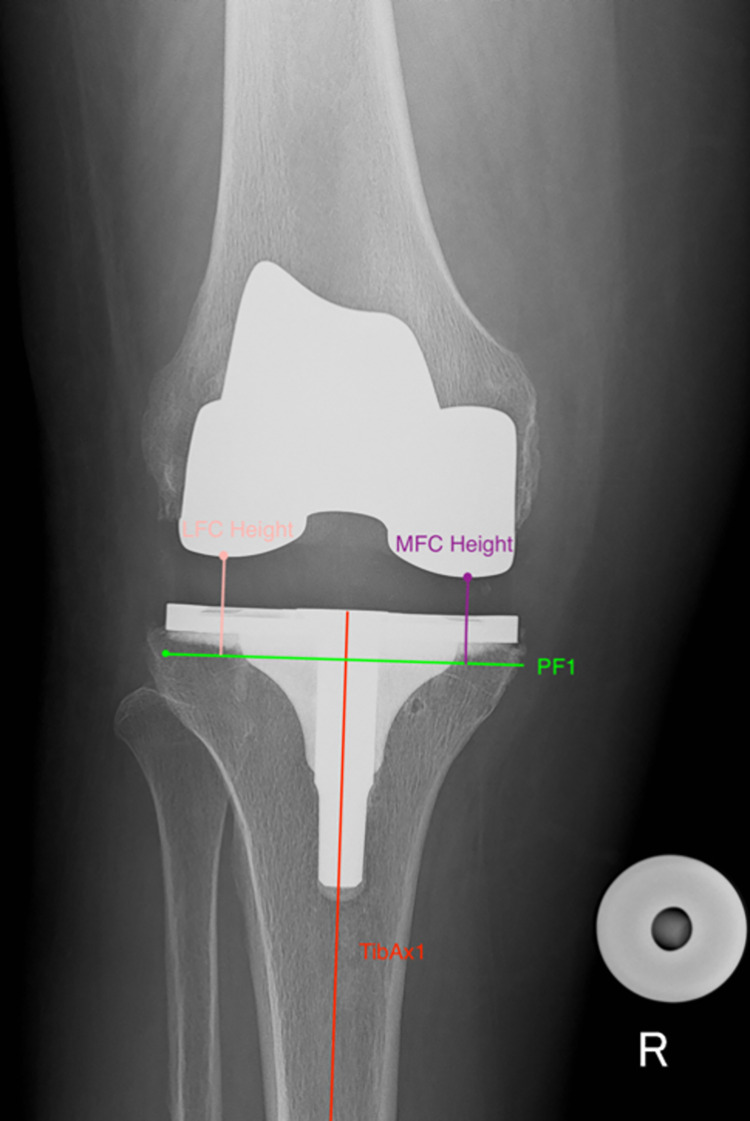
Methods: This study was a retrospective analysis of a cohort of 120 patients with end-stage knee osteoarthritis that received a TKA using the Navio Surgical System (n = 60), or Conventional manual TKA (n = 60). Procedures were performed between 1 January 2019 and 1 October 2019 at six different centres. Joint line height and posterior offset was measured pre-operatively and post-operatively on calibrated weight bearing plain radiographs of the knee. Two observers performed measurements using validated measuring tools. A BMI and age-matched cohort of patients that underwent TKA using a conventional technique in the same six centres were assessed for comparison. Mean values, standard deviations and confidence intervals are presented for change and absolute change in joint line height and posterior offset. Student's t-test was used to compare the changes between techniques.
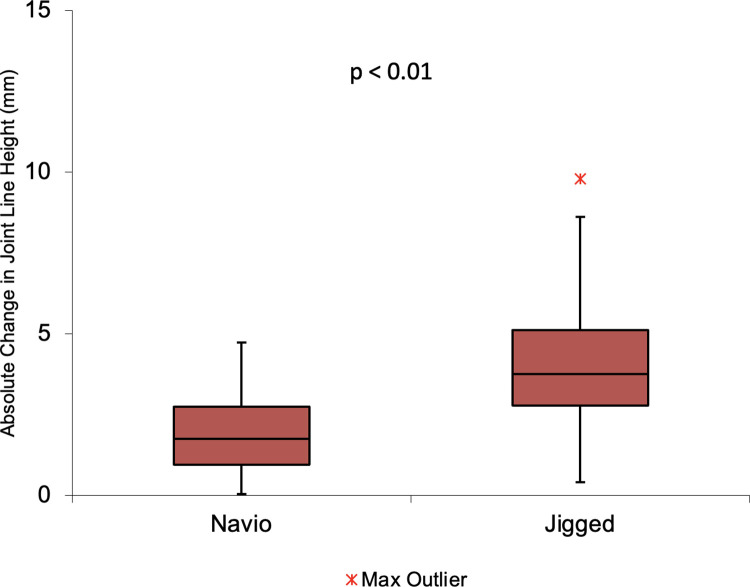
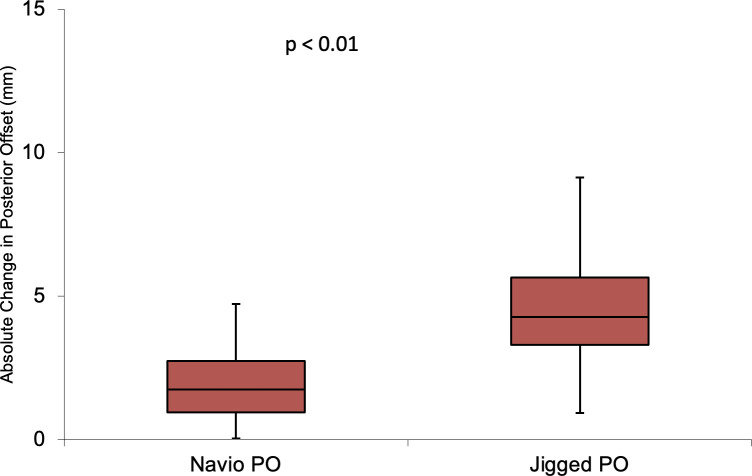
Results: Patients that underwent robotic-assisted TKA had joint line height and posterior offset restored more accurately than patients undergoing TKA using a conventional technique. Average change from pre-operative measurement in joint line height using raTKA was -0.38mm [95% CI: -0.79 to 0.03] vs 0.91 [0.14 to 1.68] with the conventional technique. Average absolute change in joint line height using raTKA was 1.96mm [1.74 to 2.18] vs 4.00mm [3.68 to 4.32] with the conventional technique. Average change in posterior offset using raTKA was 0.08mm [-0.40 to 0.56] vs 1.64mm [2.47 to 0.81] with the conventional technique. Average absolute change in posterior offset with raTKA was 2.19mm [1.92 to 2.46] vs 4.24mm [3.79 to 4.69] with the conventional technique. There was a significant difference when comparing absolute change in joint line height and posterior offset between groups (p<0.01).
Conclusion: Robotic-assisted primary TKA restores the joint line height and posterior offset more accurately than conventional jig-based techniques.
Conflict of interest statement
AA, PB, ME, SJ, JLV & DN are reimbursed for educational activities by Smith & Nephew. This does not alter our adherence to PLOS ONE policies on sharing data and materials
Figures
References
-
- Martin JW, Whiteside LA. The influence of joint line position on knee stability after condylar knee arthroplasty. Clin Orthop Relat Res. 1990. - PubMed
-
- Rota A, De Santis P, Rota P, Aureli A. Joint line restoration after primary and revision total knee arthroplasty. J Orthop Traumatol. 2013;1
-
- Partington PF, Sawhney J, Rorabeck CH, Barrack RL, Moore J. Joint line restoration after revision total knee arthroplasty. Clin Orthop Relat Res. 1999. - PubMed
-
- Ryu J, Saito S, Yamamoto K, Sano S. Factors influencing the postoperative range of motion in total knee arthroplasty. Vol. 53, Bulletin: Hosp Joint Dis. 1993. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
