

Urban-rural differences in hypertension prevalence in low-income and middle-income countries, 1990-2020: A systematic review and meta-analysis
- PMID: 36007101
- PMCID: PMC9410549
- DOI: 10.1371/journal.pmed.1004079
Urban-rural differences in hypertension prevalence in low-income and middle-income countries, 1990-2020: A systematic review and meta-analysis
Abstract
Background: The influence of urbanicity on hypertension prevalence remains poorly understood. We conducted a systematic review and meta-analysis to assess the difference in hypertension prevalence between urban and rural areas in low-income and middle-income countries (LMICs), where the most pronounced urbanisation is underway.
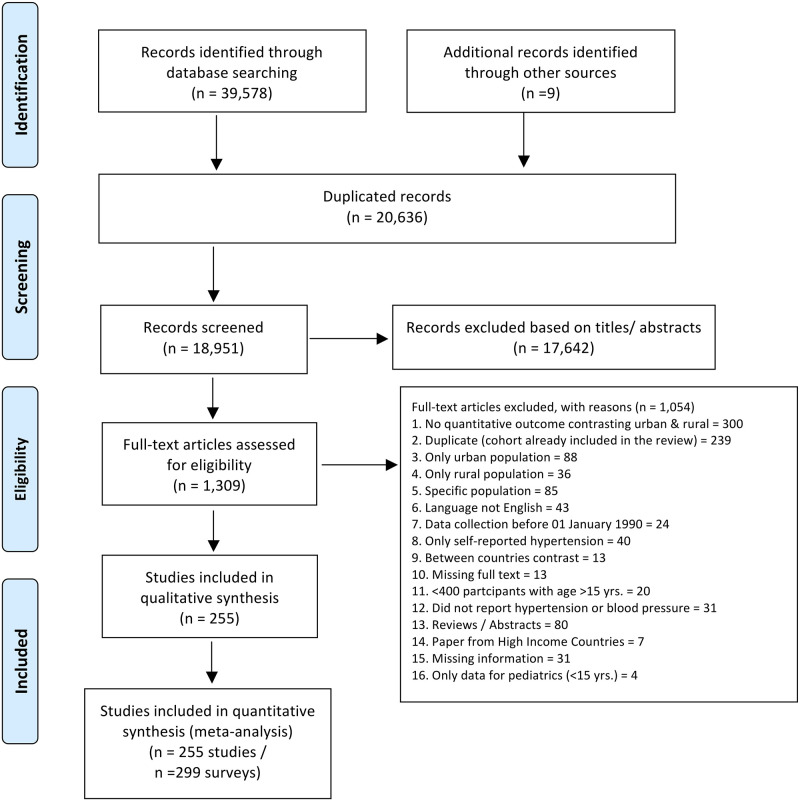
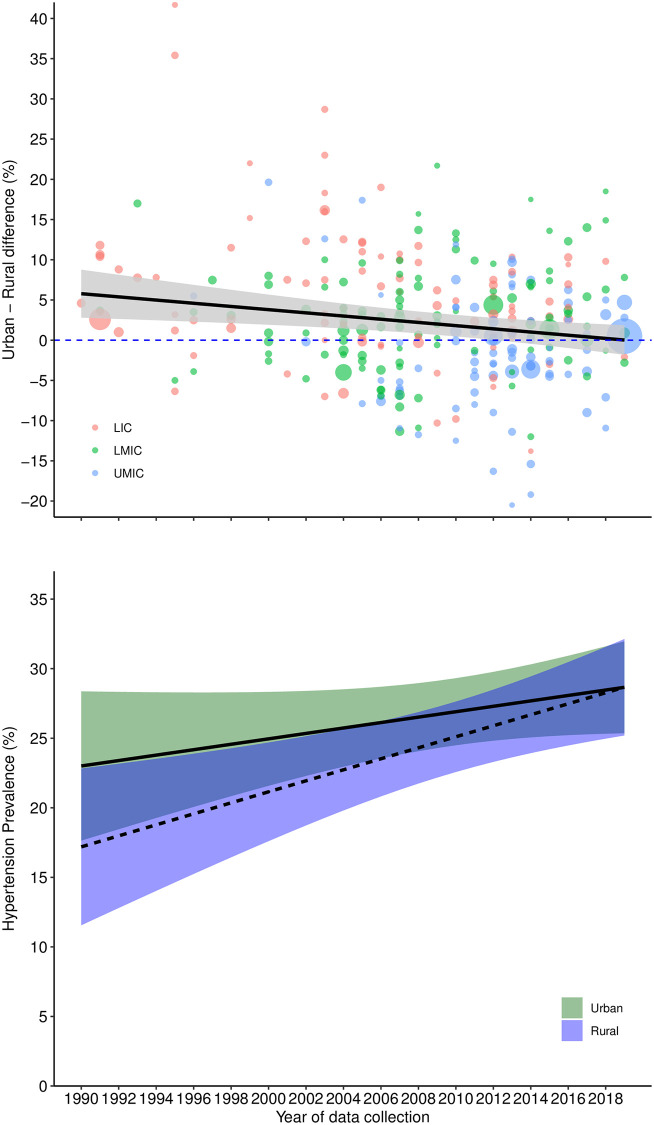
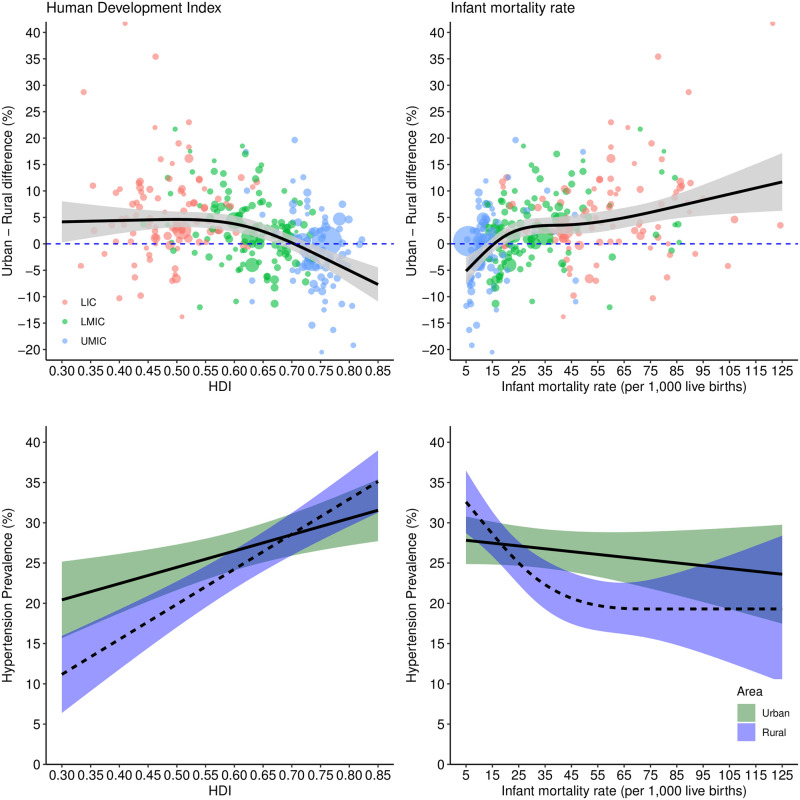
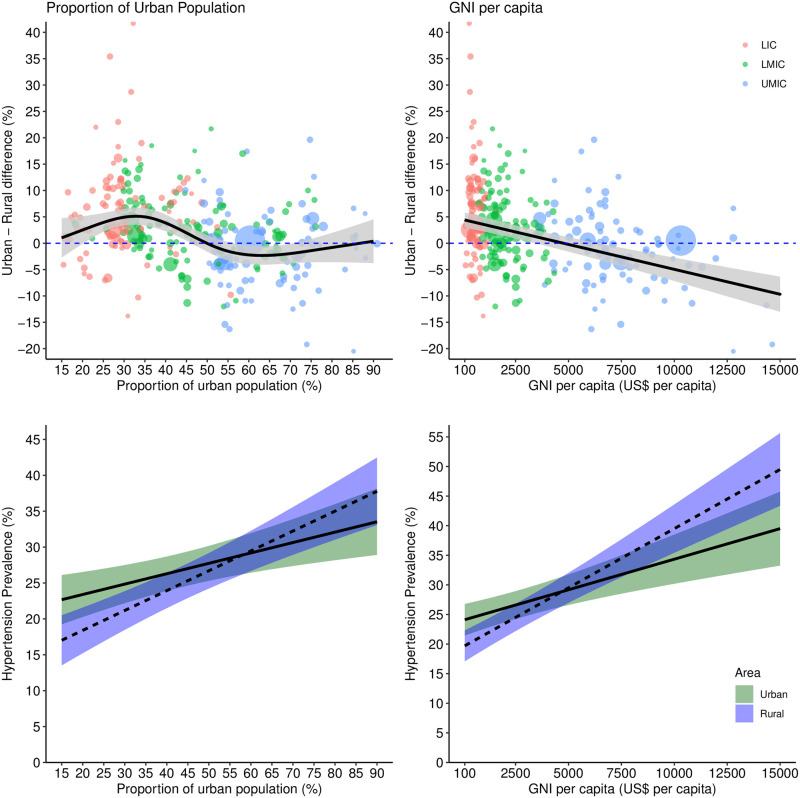
Methods and findings: We searched PubMed, Web of Science, Scopus, and Embase, from 01/01/1990 to 10/03/2022. We included population-based studies with ≥400 participants 15 years and older, selected by using a valid sampling technique, from LMICs that reported the urban-rural difference in hypertension prevalence using similar blood pressure measurements. We excluded abstracts, reviews, non-English studies, and those with exclusively self-reported hypertension prevalence. Study selection, quality assessment, and data extraction were performed by 2 independent reviewers following a standardised protocol. Our primary outcome was the urban minus rural prevalence of hypertension. Hypertension was defined as systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure as ≥90 mm Hg and could include use of antihypertensive medication, self-reported diagnosis, or both. We investigated heterogeneity using study-level and socioeconomic country-level indicators. We conducted meta-analysis and meta-regression using random-effects models. This systematic review and meta-analysis has been registered with PROSPERO (CRD42018091671). We included 299 surveys from 66 LMICs, including 19,770,946 participants (mean age 45.4 ± SD = 9 years, 53.0% females and 63.1% from rural areas). The pooled prevalence of hypertension was 30.5% (95% CI, 28.9, 32.0) in urban areas and 27.9% (95% CI, 26.3, 29.6) in rural areas, resulting in a pooled urban-rural difference of 2.45% (95% CI, 1.57, 3.33, I-square: 99.71%, tau-square: 0.00524, Pheterogeneity < 0.001). Hypertension prevalence increased over time and the rate of change was greater in rural compared to urban areas, resulting in a pooled urban-rural difference of 5.75% (95% CI, 4.02, 7.48) in the period 1990 to 2004 and 1.38% (95% CI, 0.40, 2.37) in the period 2005 to 2020, p < 0.001 for time period. We observed substantial heterogeneity in the urban-rural difference of hypertension, which was partially explained by urban-rural definition, probably high risk of bias in sampling, country income status, region, and socioeconomic indicators. The urban-rural difference was 5.67% (95% CI, 4.22, 7.13) in low, 2.74% (95% CI, 1.41, 4.07) in lower-middle and -1.22% (95% CI, -2.73, 0.28) in upper-middle-income countries in the period 1990 to 2020, p < 0.001 for country income. The urban-rural difference was highest for South Asia (7.50%, 95% CI, 5.73, 9.26), followed by sub-Saharan Africa (4.24%, 95% CI, 2.62, 5.86) and reversed for Europe and Central Asia (-6.04%, 95% CI, -9.06, -3.01), in the period 1990 to 2020, p < 0.001 for region. Finally, the urban-rural difference in hypertension prevalence decreased nonlinearly with improvements in Human Development Index and infant mortality rate. Limitations included lack of data available from all LMICs and variability in urban and rural definitions in the literature.
Conclusions: The prevalence of hypertension in LMICs increased between 1990 and 2020 in both urban and rural areas, but with a stronger trend in rural areas. The urban minus rural hypertension difference decreased with time, and with country-level socioeconomic development. Focused action, particularly in rural areas, is needed to tackle the burden of hypertension in LMICs.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. [cited 2020 Nov 26]. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30752... - PMC - PubMed
-
- Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. [cited 2020 Nov 26]. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30925... - PMC - PubMed
