

Black Fungus and beyond: COVID-19 associated infections
- PMID: 36007282
- PMCID: PMC9308173
- DOI: 10.1016/j.clinimag.2022.07.005
Black Fungus and beyond: COVID-19 associated infections
Abstract
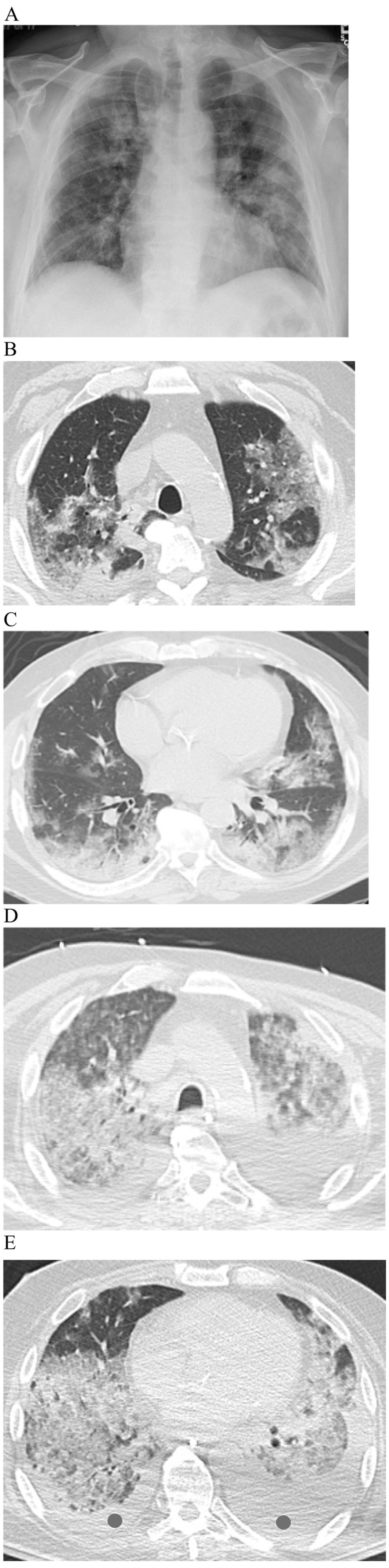
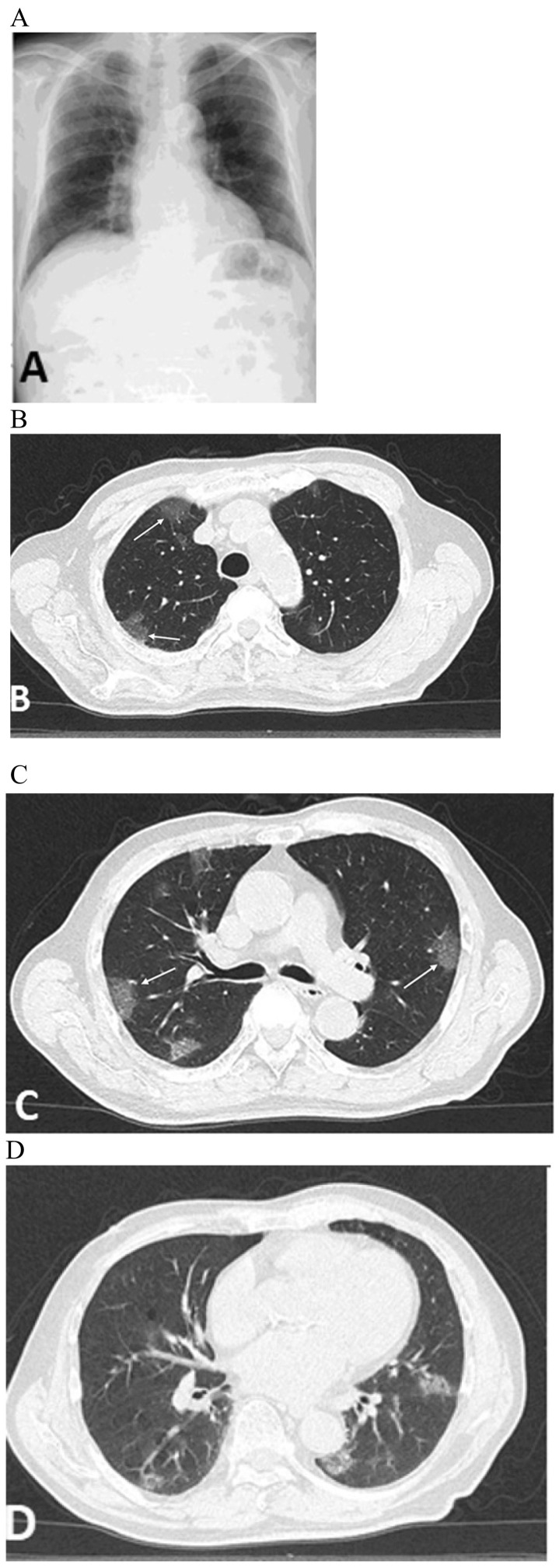
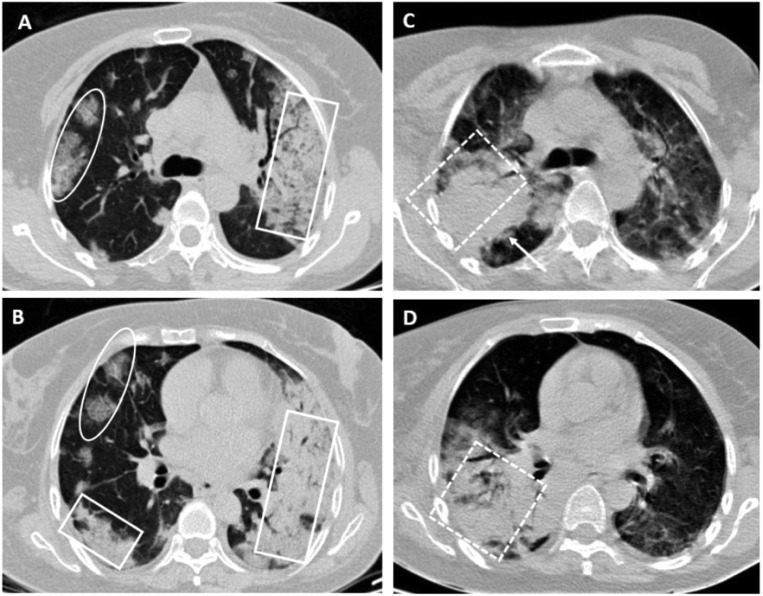
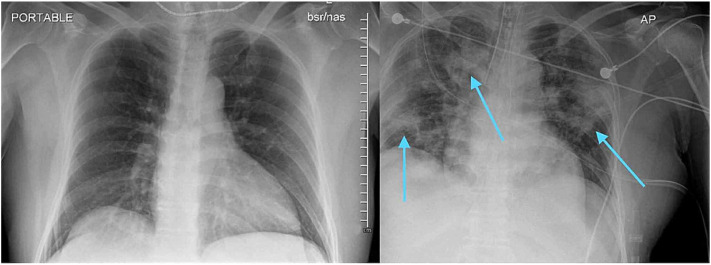
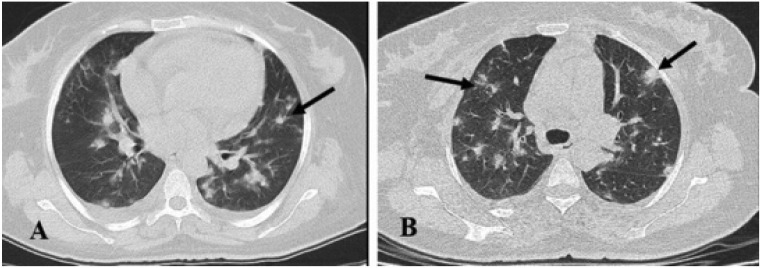
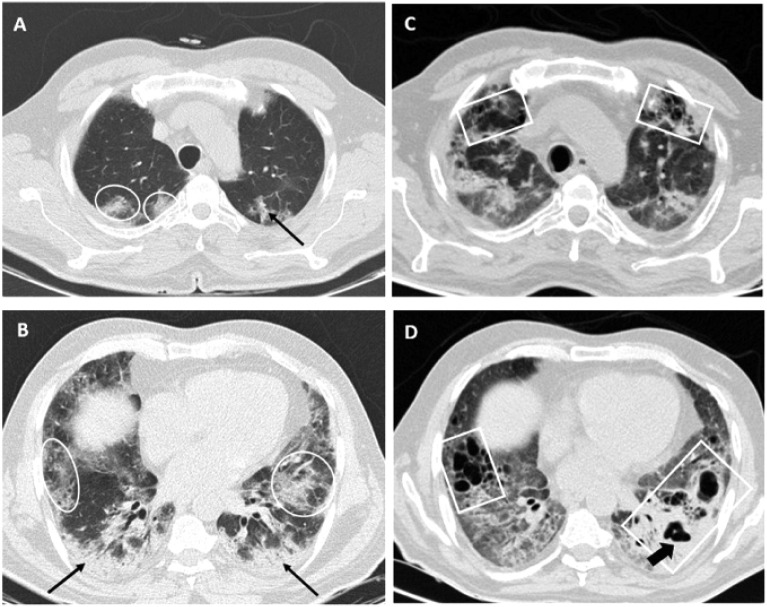
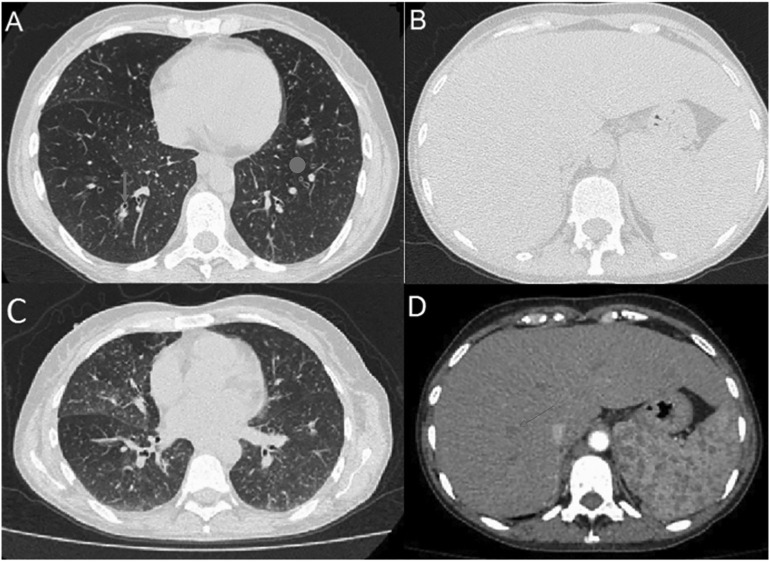
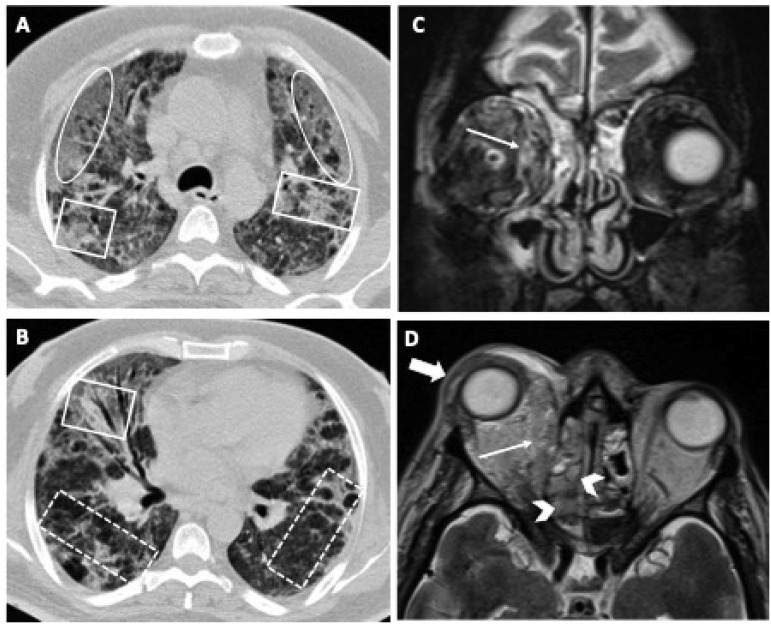
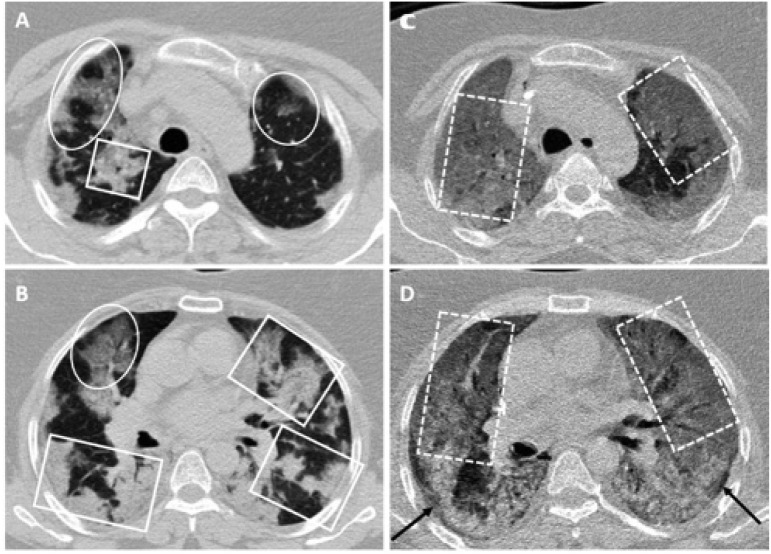
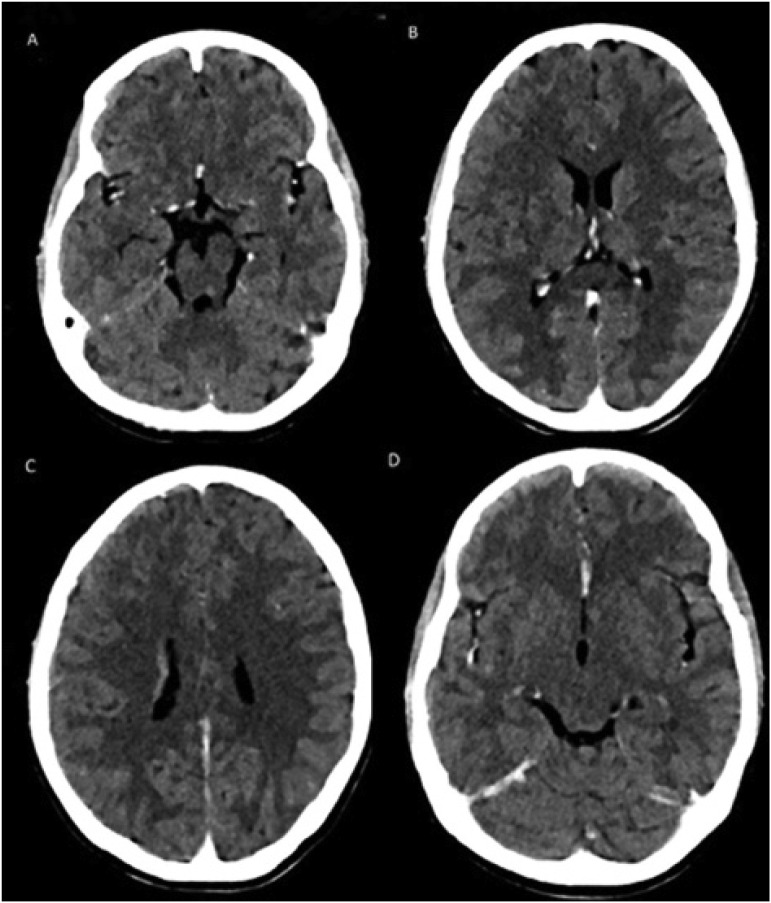
Globally, many hospitalized COVID-19 patients can experience an unexpected acute change in status, prompting rapid and expert clinical assessment. Superimposed infections can be a significant cause of clinical and radiologic deviations in this patient population, further worsening clinical outcome and muddling the differential diagnosis. As thrombotic, inflammatory, and medication-induced complications can also trigger an acute change in COVID-19 patient status, imaging early and often plays a vital role in distinguishing the cause of patient decline and monitoring patient outcome. While the common radiologic findings of COVID-19 infection are now widely reported, little is known about the clinical manifestations and imaging findings of superimposed infection. By discussing case studies of patients who developed bacterial, fungal, parasitic, and viral co-infections and identifying the most frequently reported imaging findings of superimposed infections, physicians will be more familiar with common infectious presentations and initiate a directed workup sooner. Ultimately, any abrupt changes in the expected COVID-19 imaging presentation, such as the presence of new consolidations or cavitation, should prompt further workup to exclude superimposed opportunistic infection.
Keywords: COVID-19; Co-infection; Opportunistic infection; Superimposed infection.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare they have no conflict of interest in this study.
Figures
References
-
- Hosseiny M., Kooraki S., Gholamrezanezhad A., Reddy S., Myers L. Radiology perspective of Coronavirus Disease 2019 (COVID-19): lessons from severe acute respiratory syndrome and middle east respiratory syndrome. AJR Am J Roentgenol. 2020 May;214(5):1078–1082. doi: 10.2214/AJR.20.22969. Epub 2020 Feb 28. PMID: 32108495. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
