

Single-cell analysis of hepatoblastoma identifies tumor signatures that predict chemotherapy susceptibility using patient-specific tumor spheroids
- PMID: 36008377
- PMCID: PMC9411569
- DOI: 10.1038/s41467-022-32473-z
Single-cell analysis of hepatoblastoma identifies tumor signatures that predict chemotherapy susceptibility using patient-specific tumor spheroids
Abstract
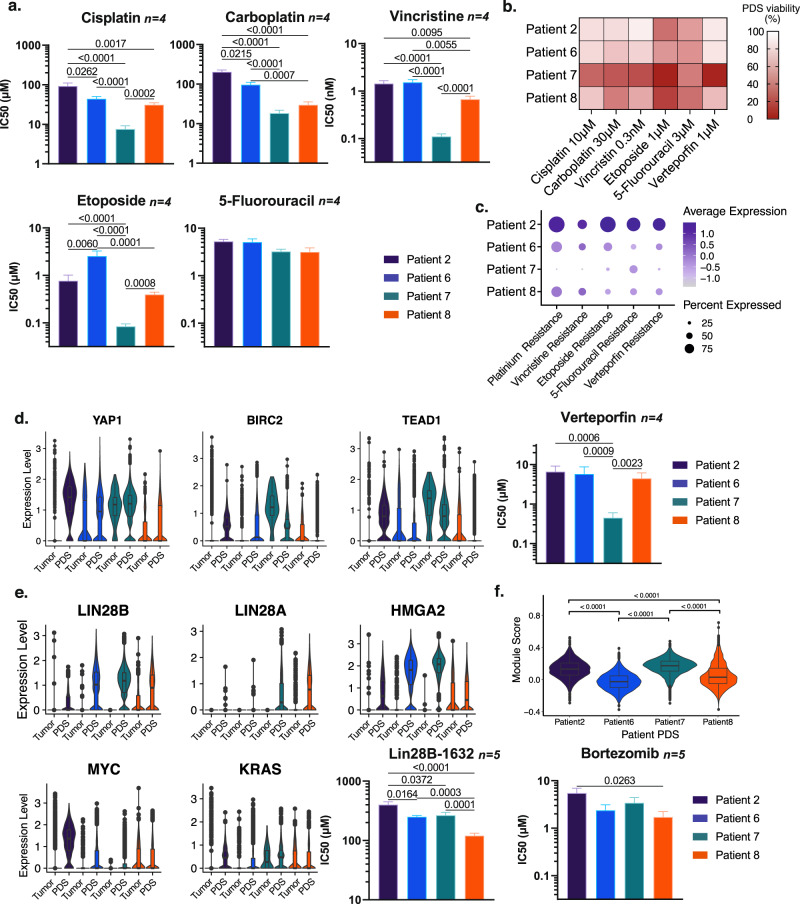
Pediatric hepatoblastoma is the most common primary liver cancer in infants and children. Studies of hepatoblastoma that focus exclusively on tumor cells demonstrate sparse somatic mutations and a common cell of origin, the hepatoblast, across patients. In contrast to the homogeneity these studies would suggest, hepatoblastoma tumors have a high degree of heterogeneity that can portend poor prognosis. In this study, we use single-cell transcriptomic techniques to analyze resected human pediatric hepatoblastoma specimens, and identify five hepatoblastoma tumor signatures that may account for the tumor heterogeneity observed in this disease. Notably, patient-derived hepatoblastoma spheroid cultures predict differential responses to treatment based on the transcriptomic signature of each tumor, suggesting a path forward for precision oncology for these tumors. In this work, we define hepatoblastoma tumor heterogeneity with single-cell resolution and demonstrate that patient-derived spheroids can be used to evaluate responses to chemotherapy.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
