

The chronification of post-COVID condition associated with neurocognitive symptoms, functional impairment and increased healthcare utilization
- PMID: 36008436
- PMCID: PMC9403954
- DOI: 10.1038/s41598-022-18673-z
The chronification of post-COVID condition associated with neurocognitive symptoms, functional impairment and increased healthcare utilization
Abstract
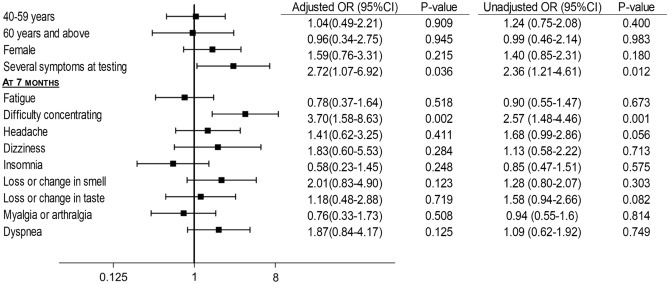
Post-COVID condition is prevalent in 10-35% of cases in outpatient settings, however a stratification of the duration and severity of symptoms is still lacking, adding to the complexity and heterogeneity of the definition of post-COVID condition and its oucomes. In addition, the potential impacts of a longer duration of disease are not yet clear, along with which risk factors are associated with a chronification of symptoms beyond the initial 12 weeks. In this study, follow-up was conducted at 7 and 15 months after testing at the outpatient SARS-CoV-2 testing center of the Geneva University Hospitals. The chronification of symptoms was defined as the continuous presence of symptoms at each evaluation timepoint (7 and 15 months). Adjusted estimates of healthcare utilization, treatment, functional impairment and quality of life were calculated. Logistic regression models were used to evaluate the associations between the chronification of symptoms and predictors. Overall 1383 participants were included, with a mean age of 44.3 years, standard deviation (SD) 13.4 years, 61.4% were women and 54.5% did not have any comorbidities. Out of SARS-CoV-2 positive participants (n = 767), 37.0% still had symptoms 7 months after their test of which 47.9% had a resolution of symptoms at the second follow-up (15 months after the infection), and 52.1% had persistent symptoms and were considered to have a chronification of their post-COVID condition. Individuals with a chronification of symptoms had an increased utilization of healthcare resources, more recourse to treatment, more functional impairment, and a poorer quality of life. Having several symptoms at testing and difficulty concentrating at 7 months were associated with a chronification of symptoms. COVID-19 patients develop post-COVID condition to varying degrees and duration. Individuals with a chronification of symptoms experience a long-term impact on their health status, functional capacity and quality of life, requiring a special attention, more involved care and early on identification considering the associated predictors.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- World Health Organization. A clinical case defintion of post COVID-19 condition by a Delphi consensus. Last updated October 6, (2021) https://apps.who.int/iris/bitstream/handle/10665/345824/WHO-2019-nCoV-Po... (Accessed 10 Oct 2021).
-
- Huang L, Yao Q, Gu X, Wang Q, Ren L, Wang Y, Hu P, Guo L, Liu M, Xu J, Zhang X, Qu Y, Fan Y, Li X, Li C, Yu T, Xia J, Wei M, Chen L, Li Y, Xiao F, Liu D, Wang J, Wang X, Cao B. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet. 2021;398(10302):747–758. doi: 10.1016/S0140-6736(21)01755-4. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
