

Nordic dietary patterns and cardiometabolic outcomes: a systematic review and meta-analysis of prospective cohort studies and randomised controlled trials
- PMID: 36008559
- PMCID: PMC9630197
- DOI: 10.1007/s00125-022-05760-z
Nordic dietary patterns and cardiometabolic outcomes: a systematic review and meta-analysis of prospective cohort studies and randomised controlled trials
Abstract
Aims/hypothesis: Nordic dietary patterns that are high in healthy traditional Nordic foods may have a role in the prevention and management of diabetes. To inform the update of the EASD clinical practice guidelines for nutrition therapy, we conducted a systematic review and meta-analysis of Nordic dietary patterns and cardiometabolic outcomes.
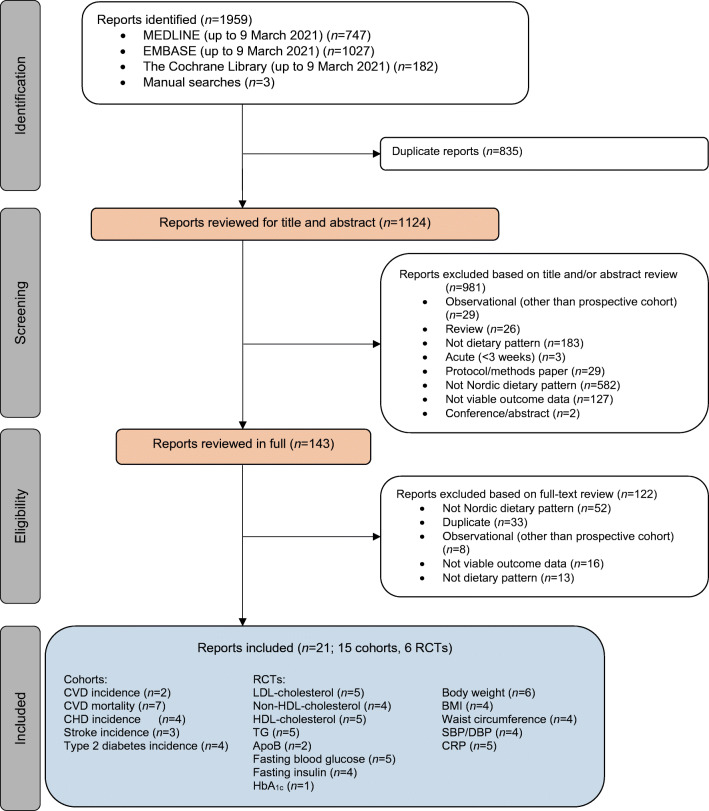
Methods: We searched MEDLINE, EMBASE and The Cochrane Library from inception to 9 March 2021. We included prospective cohort studies and RCTs with a follow-up of ≥1 year and ≥3 weeks, respectively. Two independent reviewers extracted relevant data and assessed the risk of bias (Newcastle-Ottawa Scale and Cochrane risk of bias tool). The primary outcome was total CVD incidence in the prospective cohort studies and LDL-cholesterol in the RCTs. Secondary outcomes in the prospective cohort studies were CVD mortality, CHD incidence and mortality, stroke incidence and mortality, and type 2 diabetes incidence; in the RCTs, secondary outcomes were other established lipid targets (non-HDL-cholesterol, apolipoprotein B, HDL-cholesterol, triglycerides), markers of glycaemic control (HbA1c, fasting glucose, fasting insulin), adiposity (body weight, BMI, waist circumference) and inflammation (C-reactive protein), and blood pressure (systolic and diastolic blood pressure). The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of the evidence.
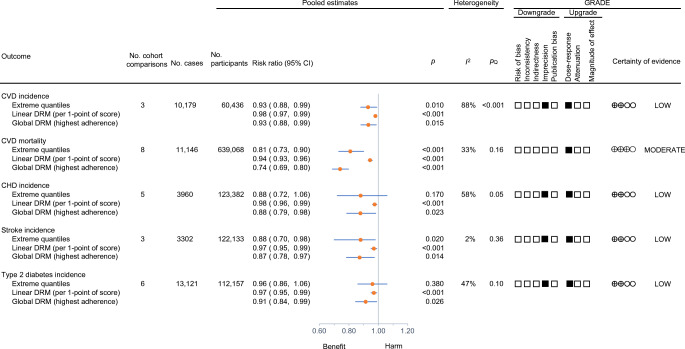
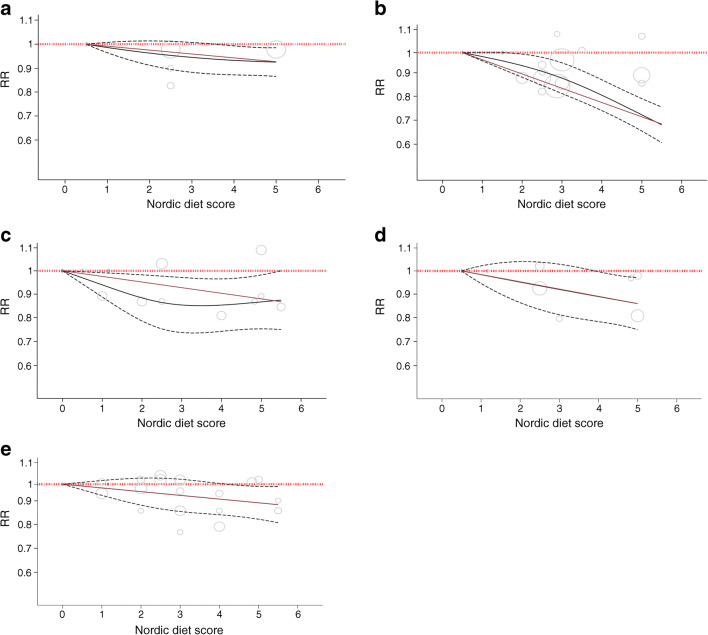
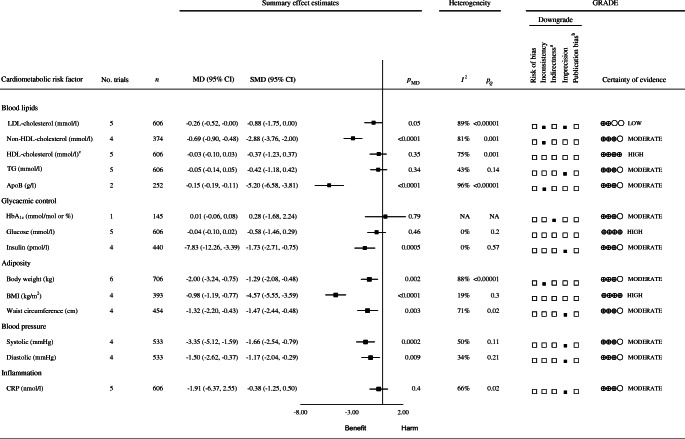
Results: We included 15 unique prospective cohort studies (n=1,057,176, with 41,708 cardiovascular events and 13,121 diabetes cases) of people with diabetes for the assessment of cardiovascular outcomes or people without diabetes for the assessment of diabetes incidence, and six RCTs (n=717) in people with one or more risk factor for diabetes. In the prospective cohort studies, higher adherence to Nordic dietary patterns was associated with 'small important' reductions in the primary outcome, total CVD incidence (RR for highest vs lowest adherence: 0.93 [95% CI 0.88, 0.99], p=0.01; substantial heterogeneity: I2=88%, pQ<0.001), and similar or greater reductions in the secondary outcomes of CVD mortality and incidence of CHD, stroke and type 2 diabetes (p<0.05). Inverse dose-response gradients were seen for total CVD incidence, CVD mortality and incidence of CHD, stroke and type 2 diabetes (p<0.05). No studies assessed CHD or stroke mortality. In the RCTs, there were small important reductions in LDL-cholesterol (mean difference [MD] -0.26 mmol/l [95% CI -0.52, -0.00], pMD=0.05; substantial heterogeneity: I2=89%, pQ<0.01), and 'small important' or greater reductions in the secondary outcomes of non-HDL-cholesterol, apolipoprotein B, insulin, body weight, BMI and systolic blood pressure (p<0.05). For the other outcomes there were 'trivial' reductions or no effect. The certainty of the evidence was low for total CVD incidence and LDL-cholesterol; moderate to high for CVD mortality, established lipid targets, adiposity markers, glycaemic control, blood pressure and inflammation; and low for all other outcomes, with evidence being downgraded mainly because of imprecision and inconsistency.
Conclusions/interpretation: Adherence to Nordic dietary patterns is associated with generally small important reductions in the risk of major CVD outcomes and diabetes, which are supported by similar reductions in LDL-cholesterol and other intermediate cardiometabolic risk factors. The available evidence provides a generally good indication of the likely benefits of Nordic dietary patterns in people with or at risk for diabetes.
Registration: ClinicalTrials.gov NCT04094194.
Funding: Diabetes and Nutrition Study Group of the EASD Clinical Practice.
Keywords: Cardiovascular disease; Meta-analysis; Nordic diet; Prospective cohort; Randomised controlled trial; Systematic review.
© 2022. The Author(s).
Figures
References
-
- Becerra-Tomas N, Blanco Mejia S, Viguiliouk E, et al. Mediterranean diet, cardiovascular disease and mortality in diabetes: A systematic review and meta-analysis of prospective cohort studies and randomized clinical trials. Crit Rev Food Sci Nutr. 2020;60(7):1207–1227. doi: 10.1080/10408398.2019.1565281. - DOI - PubMed
-
- Elhayany A, Lustman A, Abel R, Attal-Singer J, Vinker S. A low carbohydrate Mediterranean diet improves cardiovascular risk factors and diabetes control among overweight patients with type 2 diabetes mellitus: a 1-year prospective randomized intervention study. Diabetes Obes Metab. 2010;12(3):204–209. doi: 10.1111/j.1463-1326.2009.01151.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
