

Object-centered sensorimotor bias of torque control in the chronic stage following stroke
- PMID: 36008561
- PMCID: PMC9411611
- DOI: 10.1038/s41598-022-18754-z
Object-centered sensorimotor bias of torque control in the chronic stage following stroke
Abstract
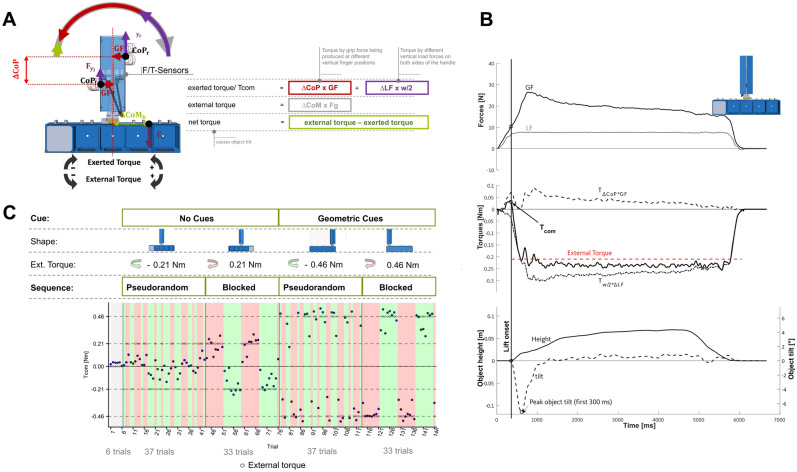
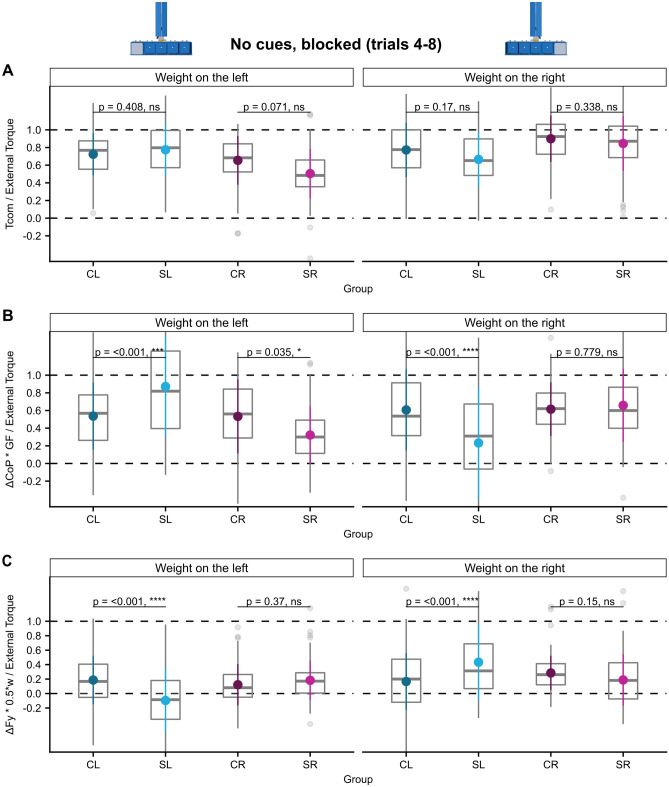
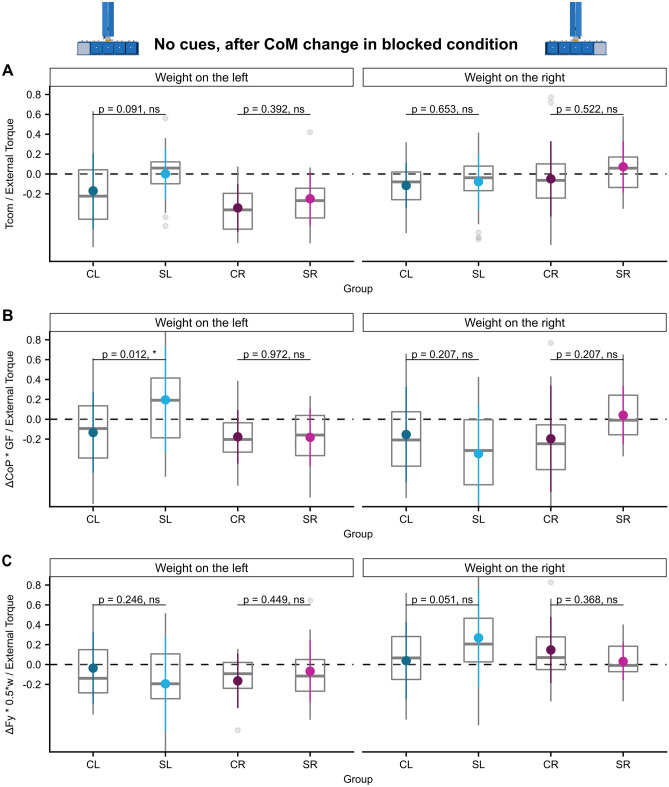
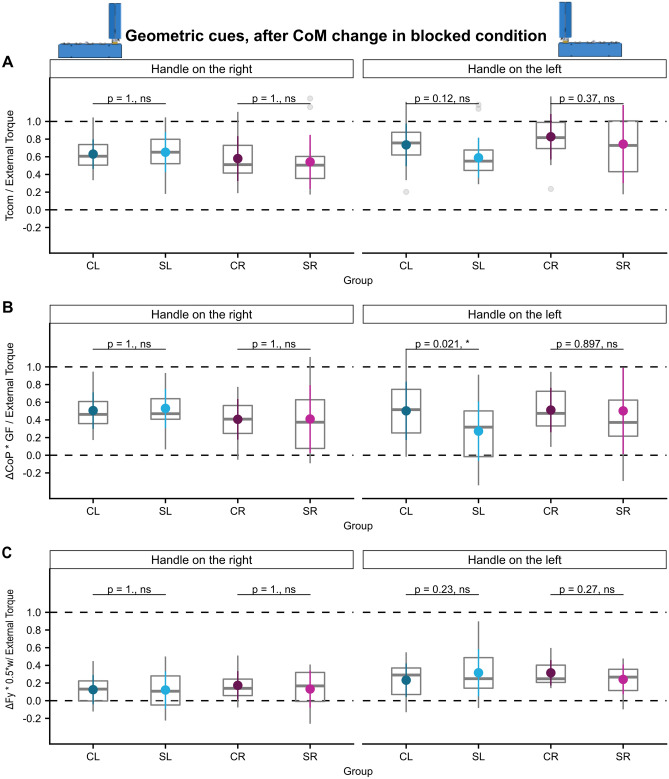
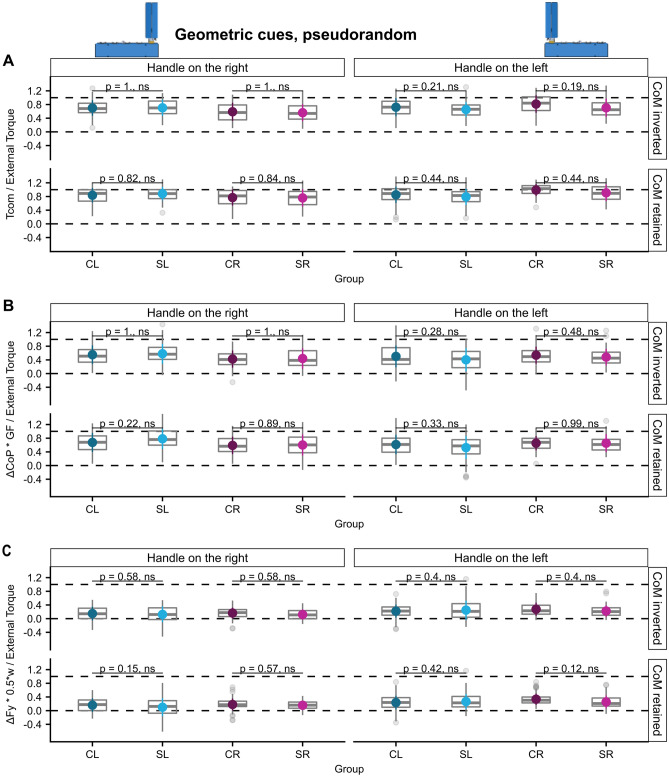
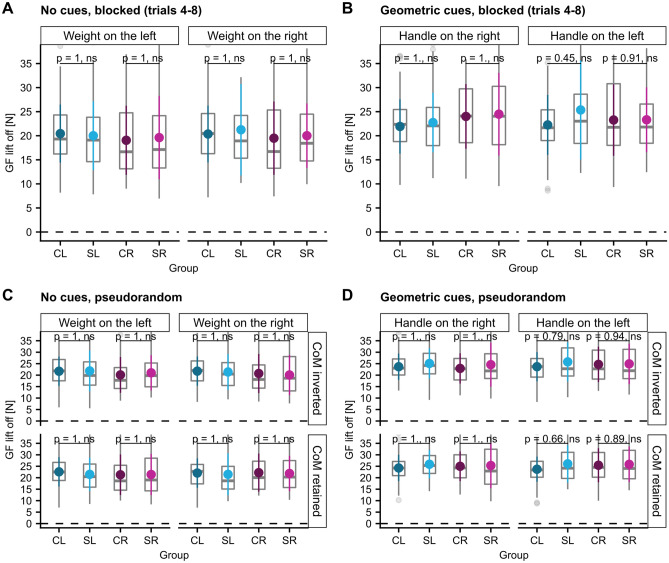
When lifting objects whose center of mass (CoM) are not centered below the handle one must compensate for arising external torques already at lift-off to avoid object tilt. Previous studies showed that finger force scaling during object lifting may be impaired at both hands following stroke. However, torque control in object manipulation has not yet been studied in patients with stroke. In this pilot study, thirteen patients with chronic stage left hemispheric stroke (SL), nine patients with right hemispheric stroke (SR) and hand-matched controls had to grasp and lift an object with the fingertips of their ipsilesional hand at a handle while preventing object tilt. Object CoM and therewith the external torque was varied by either relocating a covert weight or the handle. The compensatory torque at lift-off (Tcom) is the sum of the torque resulting from (1) grip force being produced at different vertical finger positions (∆CoP × GF) and (2) different vertical load forces on both sides of the handle (∆Fy × w/2). When having to rely on sensorimotor memories, ∆CoP × GF was elevated when the object CoM was on the ipsilesional-, but decreased when CoM was on the contralesional side in SL, whereas ∆Fy × w/2 was biased in the opposite direction, resulting in normal Tcom. SR patients applied a smaller ∆CoP × GF when the CoM was on the contralesional side. Torques were not altered when geometric cues were available. Our findings provide evidence for an object-centered spatial bias of manual sensorimotor torque control with the ipsilesional hand following stroke reminiscent of premotor neglect. Both intact finger force-to-position coordination and visuomotor control may compensate for the spatial sensorimotor bias in most stroke patients. Future studies will have to confirm the found bias and evaluate the association with premotor neglect.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
