

Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: a randomized, controlled, double-blind phase 3 trial
- PMID: 36008722
- PMCID: PMC9671806
- DOI: 10.1038/s41591-022-01977-y
Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: a randomized, controlled, double-blind phase 3 trial
Abstract
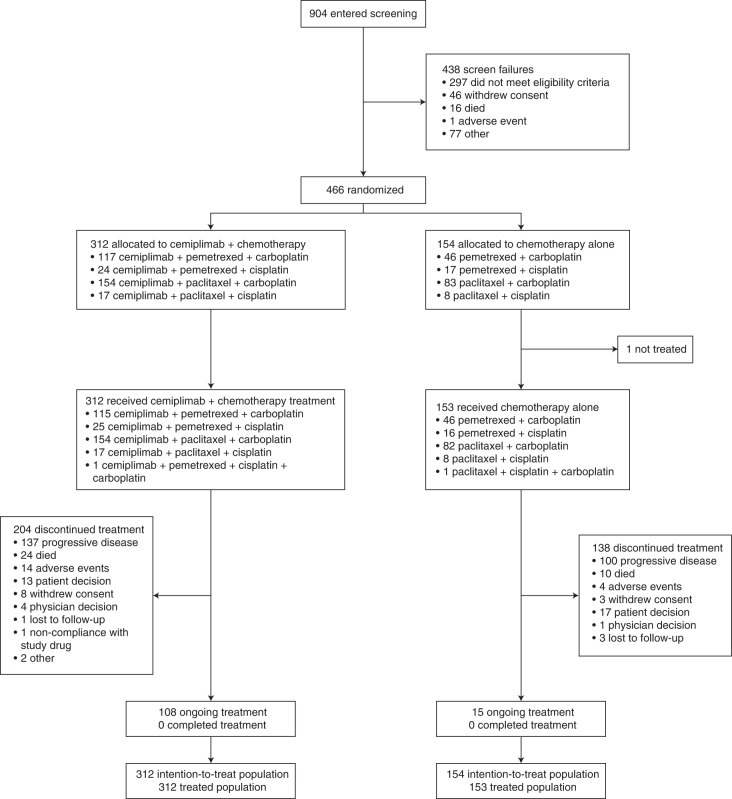
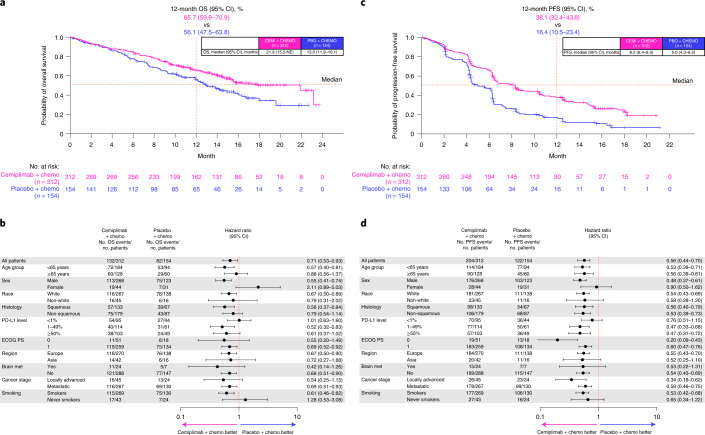
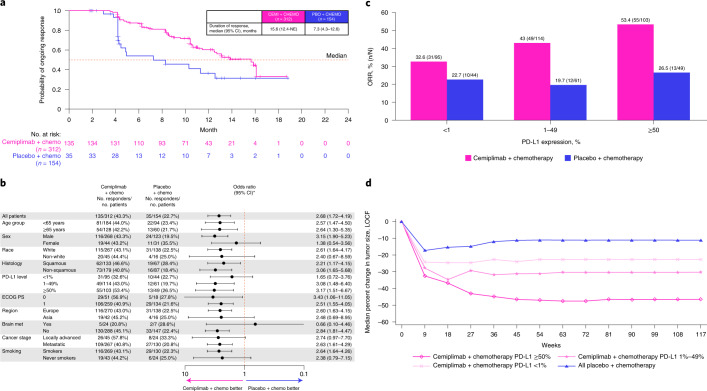
First-line cemiplimab (anti-programmed cell death-1 (PD-1)) monotherapy has previously shown significant improvement in overall survival (OS) and progression-free survival (PFS) versus chemotherapy in patients with advanced non-small cell lung cancer (aNSCLC) and PD-ligand 1 (PD-L1) expression ≥50%. EMPOWER-Lung 3 ( NCT03409614 ), a double-blind, placebo-controlled, phase 3 study, examined cemiplimab plus platinum-doublet chemotherapy as first-line treatment for aNSCLC, irrespective of PD-L1 expression or histology. In this study, 466 patients with stage III/IV aNSCLC without EGFR, ALK or ROS1 genomic tumor aberrations were randomized (2:1) to receive cemiplimab 350 mg (n = 312) or placebo (n = 154) every 3 weeks for up to 108 weeks in combination with four cycles of platinum-doublet chemotherapy (followed by pemetrexed maintenance as indicated). In total, 57.1% (266/466 patients) had non-squamous NSCLC, and 85.2% (397/466 patients) had stage IV disease. The primary endpoint was OS. The trial was stopped early per recommendation of the independent data monitoring committee, based on meeting preset OS efficacy criteria: median OS was 21.9 months (95% confidence interval (CI), 15.5-not evaluable) with cemiplimab plus chemotherapy versus 13.0 months (95% CI, 11.9-16.1) with placebo plus chemotherapy (hazard ratio (HR) = 0.71; 95% CI, 0.53-0.93; P = 0.014). Grade ≥3 adverse events occurred with cemiplimab plus chemotherapy (43.6%, 136/312 patients) and placebo plus chemotherapy (31.4%, 48/153 patients). Cemiplimab is only the second anti-PD-1/PD-L1 agent to show efficacy in aNSCLC as both monotherapy and in combination with chemotherapy for both squamous and non-squamous histologies.
© 2022. The Author(s).
Conflict of interest statement
M.G., T. Melkadze, T. Makharadze, D.G., M.D., K.L., G.N., M.N., I.R. and B.M.-J. report no conflicts of interest. K.P. reports honoraria from AstraZeneca, Merck Sharp & Dohme, Nektar, Pfizer, Regeneron Pharmaceuticals and Roche and a consulting or advisory role with Nektar. E.K. reports honoraria from Merck Sharp & Dohme, Bristol Myers Squibb, Nektar, Pfizer, Roche, AstraZeneca, Amgen and Regeneron Pharmaceuticals. C.G. reports advisory board fees or honoraria from GlaxoSmithKline, Pfizer, AstraZeneca, Roche, Novartis, Bristol Myers Squibb, Merck Sharp & Dohme, Berlin-Chemie, Chiesi, Boehringer Ingelheim and Sanofi. R.P. reports advisory board or speaker roles for Astellas, Bristol Myers Squibb, Ipsen, Janssen, Merck Sharp & Dohme, Roche and Sanofi-Aventis and institutional funding for research projects from Amgen, AstraZeneca, Novartis and Pierre-Fabre. S.L., K.M., A.P., R.G.W.Q., B.G., F.S., D.M.W., G.D.Y., I.L., G.G. and P.R. are employees and shareholders of Regeneron Pharmaceuticals.
Figures
References
-
- National Comprehensive Cancer Network. Clinical practice guidelines in oncology: non-small cell lung cancer. Version 6.2021. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf (2021).
-
- Merck Sharp & Dohme Corp. KEYTRUDA (pembrolizumab) injection, for intravenous use (US prescribing information). https://www.merck.com/product/usa/pi_circulars/k/keytruda/keytruda_pi.pdf (2021).
-
- Genentech, Inc. TECENTRIQ (atezolizumab) injection, for intravenous use (US prescribing information). https://www.gene.com/download/pdf/tecentriq_prescribing.pdf (2021).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
