An official website of the United States government
The .gov means it’s official.
Federal government websites often end in .gov or .mil. Before
sharing sensitive information, make sure you’re on a federal
government site.
The site is secure.
The https:// ensures that you are connecting to the
official website and that any information you provide is encrypted
and transmitted securely.
The native bursa is a structure lined by synovium located adjacent to a joint which may serve to decrease friction between the tendons and overlying bone or skin. This extra-articular structure can become inflamed resulting in bursitis. Steroid injections have proven to be an effective method of treating bursal pathology in various anatomic locations. Performing these procedures requires a thorough understanding of relevant anatomy, proper technique, and expected outcomes. Ultrasound is a useful tool for pre procedure diagnostic evaluation and optimizing needle position during these procedures while avoiding adjacent structures. The purpose of this article is to review core principles of ultrasound-guided musculoskeletal procedures involving bursae throughout the upper and lower extremities.
Kevin McGill is a consultant for Teleflex. The remaining authors declare no competing interests.
Figures
Fig. 1
Subacromial bursa injection. Findings: long…
Fig. 1
Subacromial bursa injection. Findings: long axis view of the supraspinatus tendon (St) before…
Fig. 1
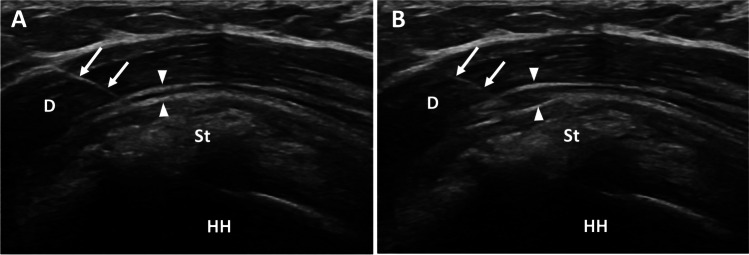
Subacromial bursa injection. Findings: long axis view of the supraspinatus tendon (St) before (A) and after (B) injection of local anesthetic into the subacromial/subdeltoid bursa outlined by thin echogenic peribursal fat (arrowheads). The needle (arrows) traverses the deltoid (D) muscle with tip located within the bursa superficial to the supraspinatus tendon (St) and humeral head (HH). The supraspinatus tendon contains echogenic calcifications, consistent with calcium hydroxyapatite deposition
Fig. 2
a Scapulothoracic bursitis. Findings: axial…
Fig. 2
a Scapulothoracic bursitis. Findings: axial T2 fat-saturated (A) and T1 fat-saturated post-contrast (B)…
Fig. 2
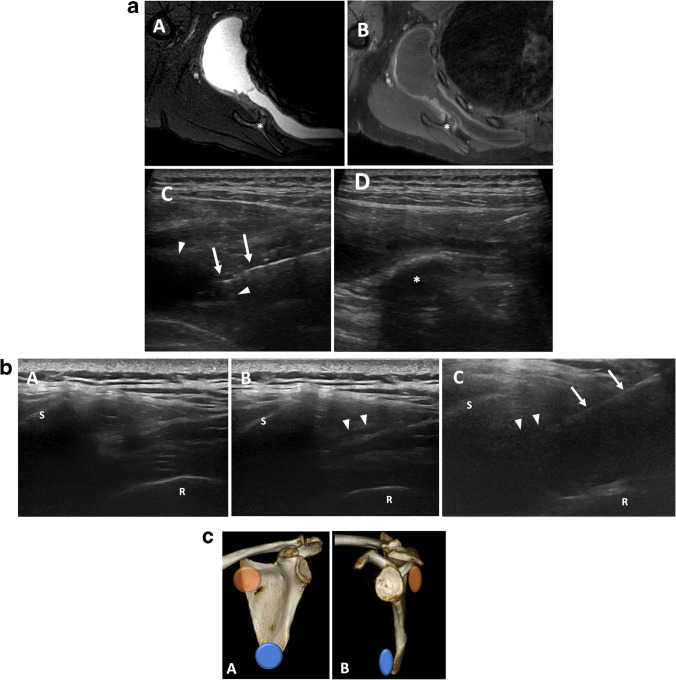
a Scapulothoracic bursitis. Findings: axial T2 fat-saturated (A) and T1 fat-saturated post-contrast (B) MRI of the shoulder with large scapulothoracic bursal effusion secondary to osteochondroma (asterisk). Ultrasound prior to aspiration (C) demonstrates needle (arrows) within the heterogenous fluid collection within the bursa (arrowheads). Post-aspiration ultrasound image (D) shows near complete resolution of fluid adjacent to the osteochondroma (asterisk). b Scapulothoracic bursal fluid with dynamic maneuver. Findings: with the transducer in transverse over the medial scapula, the scapula margin (S) and adjacent rib (R) are visualized. A patient with scapulothoracic pain demonstrates no sonographic abnormality with arm at side (A). When the arm is flexed behind the back (B), a small amount of fluid is visualized in the scapulothoracic bursa (arrowheads) confirming the diagnosis of scapulothoracic bursitis. The arm remains flexed during steroid injection (C) with needle (arrow) trajectory nearly parallel to scapula. c Major scapulothoracic bursae. Findings: three-dimensional frontal and lateral images of the scapula demonstrating the anatomic locations of the major scapulothoracic bursae. Inferaserratus/scapulothoracic bursa (blue), supraserratus/subscapularis bursa (orange)
Fig. 3
a Psoas bursal effusion. Findings:…
Fig. 3
a Psoas bursal effusion. Findings: transverse grayscale ultrasound of the hip (A) demonstrates…
Fig. 3
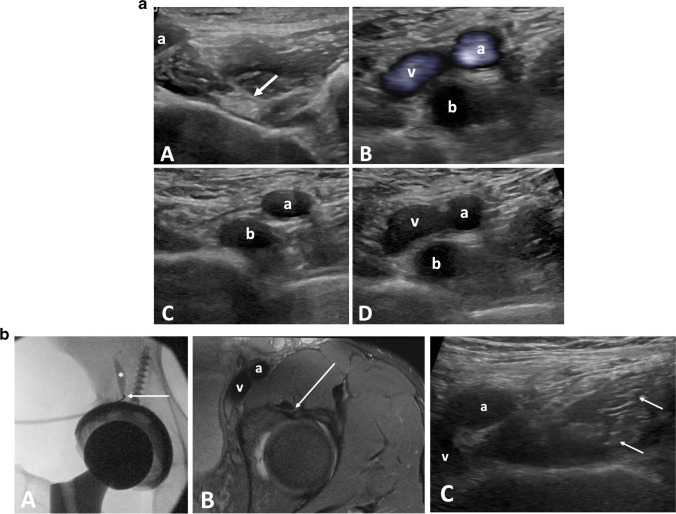
a Psoas bursal effusion. Findings: transverse grayscale ultrasound of the hip (A) demonstrates a normal psoas tendon (arrow) and femoral artery (a). Transverse views (B), (C), and (D) of the hip in a patient with a bursal effusion. In (B), Power Doppler images demonstrates a bursal effusion (b) with flow in the adjacent femoral artery (a) and vein (v). (C) and (D) were obtained with and without compression. In (C) the vein is compressed while the bursal effusion is unchanged. b Iliopsoas tendon sheath injection. Findings: fluoroscopic images of the right hip (A) in a patient with a total hip arthroplasty during iliopsoas bursa injection. Contrast (asterisk) moves superiorly away from the needle (arrow) confirming location of the within the iliopsoas bursa. Axial T2 fat-saturated and transverse ultrasound images (B and C) of the left hip on a different patients demonstrate the needle trajectory (arrow) during an ultrasound guided injection
Fig. 4
a Trochanteric bursitis. Findings: rotated…
Fig. 4
a Trochanteric bursitis. Findings: rotated Axial T2 fat saturated MRI of the hip…
Fig. 4
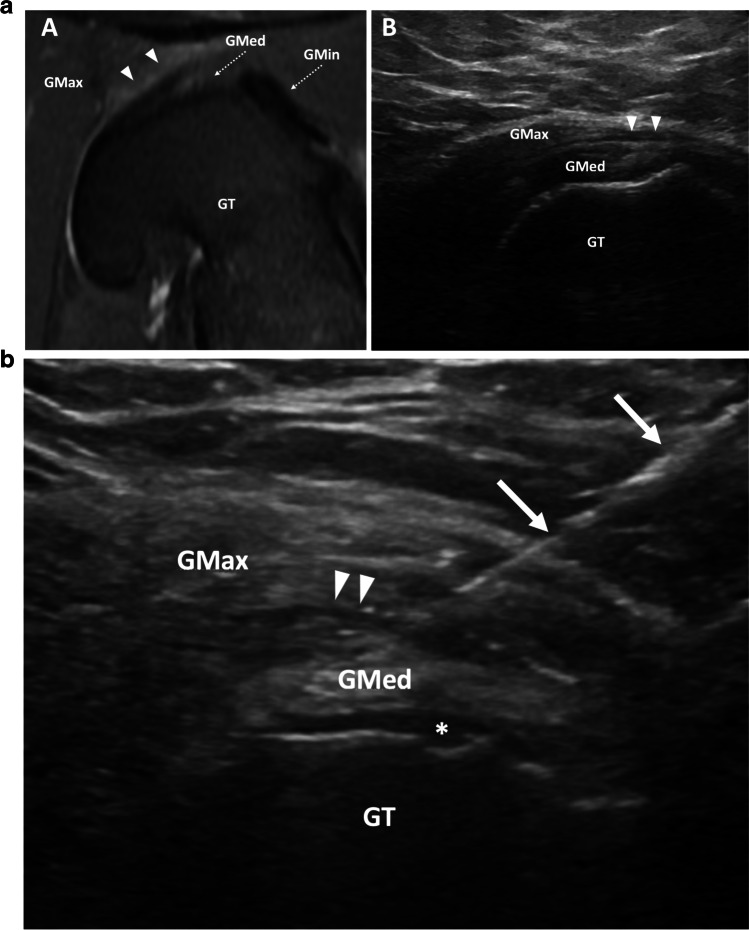
a Trochanteric bursitis. Findings: rotated Axial T2 fat saturated MRI of the hip (A) demonstrates edema-like signal in the greater trochanteric bursa (arrowheads) between the gluteus medius (GMed, dashed arrow) and gluteus maximus (GMax) overlying the greater trochanter (GT). Transverse sonographic view of the lateral hip (B) demonstrates trace fluid within the greater trochanteric bursa (arrowheads). Fluid is not frequently visualized in patients for whom greater trochanter bursa injection is requested. Gmin, gluteus minimus (dashed arrow). b Trochanteric bursa injection. Transverse ultrasound of the lateral hip demonstrates injection of fluid into the trochanteric bursa (arrowheads). Fluid in the subgluteus medius bursa (asterisk). Needle (arrows), GT, greater trochanter; GMax, gluteus maximus; GMed, gluteus medius
Fig. 5
Ischial bursitis. Findings: rotated axial…
Fig. 5
Ischial bursitis. Findings: rotated axial T2 fat-saturated ( A ) and T1 fat-saturated…
Fig. 5
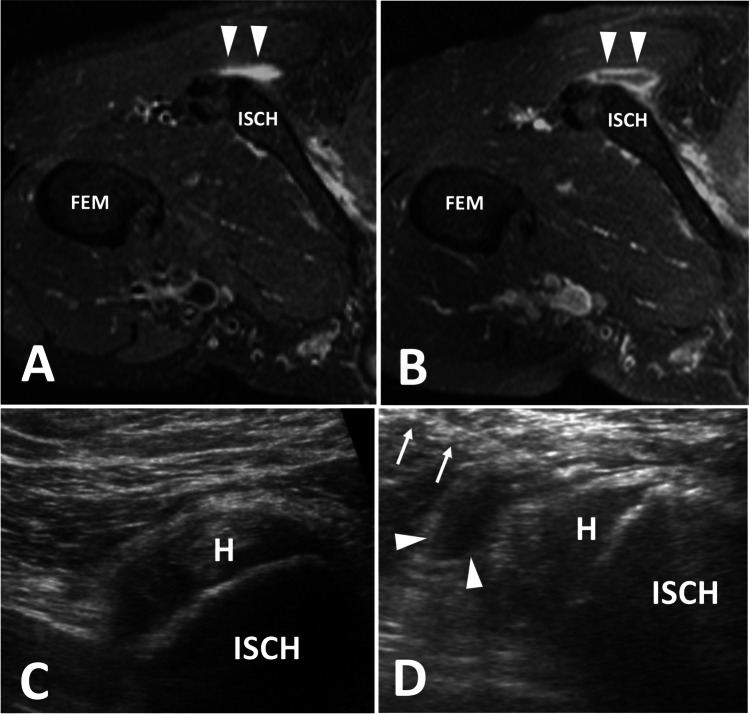
Ischial bursitis. Findings: rotated axial T2 fat-saturated (A) and T1 fat-saturated post contrast (B) images demonstrate a rim enhancing fluid collection adjacent to the ischial tuberosity within the ischial bursa, which is consistent with ischial bursitis. Transverse ultrasound images (C) of a different patient show the injection of echogenic steroids into the ischial bursa (arrowhead). H, hamstring origin; ISCH, ischial tuberosity; Fem, femur; needle (arrows)
Fig. 6
Popliteal cyst aspiration. Findings: axial…
Fig. 6
Popliteal cyst aspiration. Findings: axial T2 fat-saturated image ( A ) of the…
Fig. 6
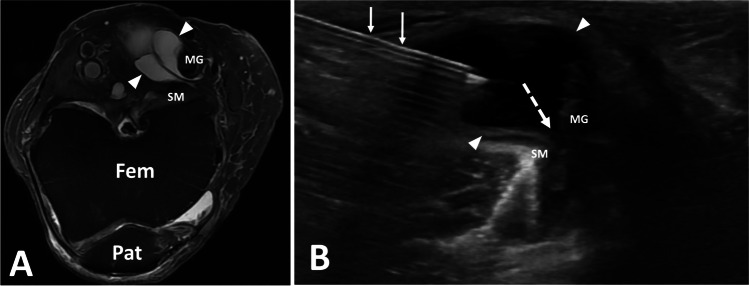
Popliteal cyst aspiration. Findings: axial T2 fat-saturated image (A) of the left knee with septated popliteal cyst (arrowheads). Transverse ultrasound image of the posterior knee during popliteal cyst aspiration show cyst extending toward knee joint (dashed arrow). Needle (arrow), Fem, femur; Pat, patella; SM, semimembranosus; MG, medial gastrocnemius
Sharpe RE, Jr, Nazarian LN, Levin DC, Parker L, Rao VM. The increasing role of nonradiologists in performing ultrasound-guided invasive procedures. J Am Coll Radiol. 2013;10(11):859–863. doi: 10.1016/j.jacr.2013.04.016.
-
DOI
-
PubMed
Kanesa-Thasan RM, Nazarian LN, Parker L, Rao VM, Levin DC. Comparative trends in utilization of MRI and Ultrasound to evaluate nonspine joint disease 2003 to 2015. J Am Coll Radiol. 2018;15(3 Pt A):402–407. doi: 10.1016/j.jacr.2017.10.015.
-
DOI
-
PubMed
Gyftopoulos S, Harkey P, Hemingway J, Hughes DR, Rosenkrantz AB, Duszak R., Jr Changing musculoskeletal extremity imaging utilization from 1994 through 2013: a Medicare beneficiary perspective. AJR Am J Roentgenol. 2017;209(5):1103–1109. doi: 10.2214/AJR.17.18346.
-
DOI
-
PubMed
Patel IJ, Rahim S, Davidson JC, Hanks SE, Tam AL, Walker TG, et al. J Vasc Interv Radiol. 2019;30(8):1168–1184 e1161. doi: 10.1016/j.jvir.2019.04.017.
-
DOI
-
PubMed
MacMahon PJ, Eustace SJ, Kavanagh EC. Injectable corticosteroid and local anesthetic preparations: a review for radiologists. Radiology. 2009;252(3):647–661. doi: 10.1148/radiol.2523081929.
-
DOI
-
PubMed