

A Bayesian reanalysis of the Standard versus Accelerated Initiation of Renal-Replacement Therapy in Acute Kidney Injury (STARRT-AKI) trial
- PMID: 36008827
- PMCID: PMC9404618
- DOI: 10.1186/s13054-022-04120-y
A Bayesian reanalysis of the Standard versus Accelerated Initiation of Renal-Replacement Therapy in Acute Kidney Injury (STARRT-AKI) trial
Abstract
Background: Timing of initiation of kidney-replacement therapy (KRT) in critically ill patients remains controversial. The Standard versus Accelerated Initiation of Renal-Replacement Therapy in Acute Kidney Injury (STARRT-AKI) trial compared two strategies of KRT initiation (accelerated versus standard) in critically ill patients with acute kidney injury and found neutral results for 90-day all-cause mortality. Probabilistic exploration of the trial endpoints may enable greater understanding of the trial findings. We aimed to perform a reanalysis using a Bayesian framework.
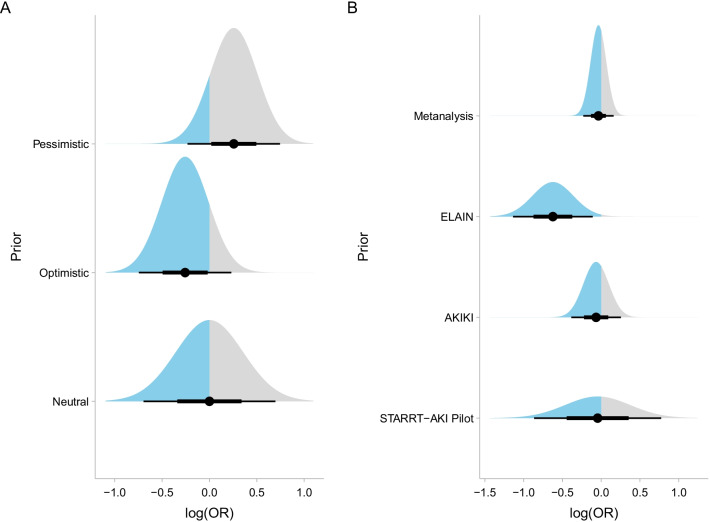
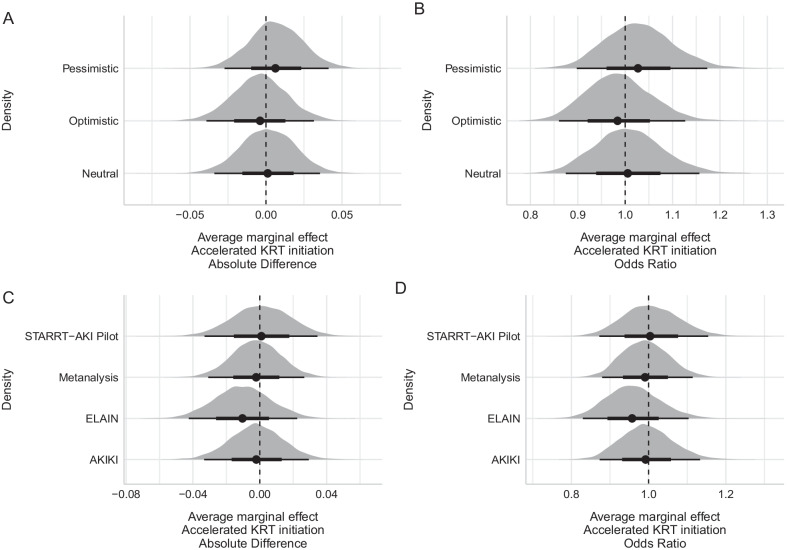
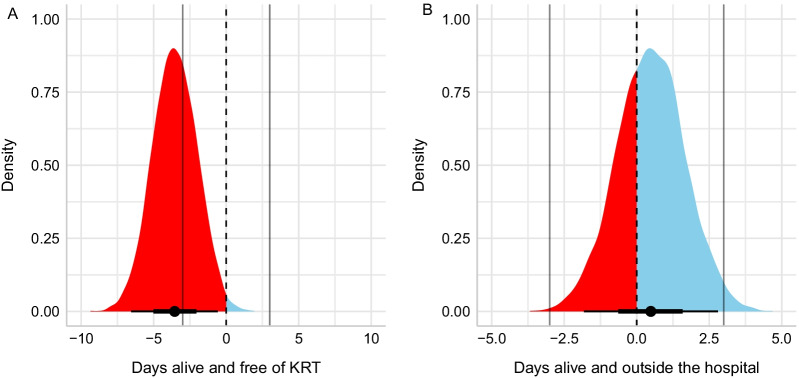
Methods: We performed a secondary analysis of all 2927 patients randomized in multi-national STARRT-AKI trial, performed at 168 centers in 15 countries. The primary endpoint, 90-day all-cause mortality, was evaluated using hierarchical Bayesian logistic regression. A spectrum of priors includes optimistic, neutral, and pessimistic priors, along with priors informed from earlier clinical trials. Secondary endpoints (KRT-free days and hospital-free days) were assessed using zero-one inflated beta regression.
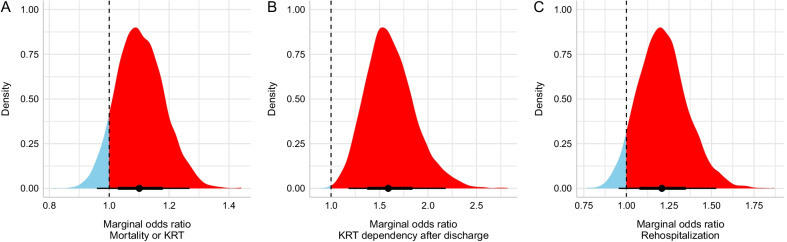
Results: The posterior probability of benefit comparing an accelerated versus a standard KRT initiation strategy for the primary endpoint suggested no important difference, regardless of the prior used (absolute difference of 0.13% [95% credible interval [CrI] - 3.30%; 3.40%], - 0.39% [95% CrI - 3.46%; 3.00%], and 0.64% [95% CrI - 2.53%; 3.88%] for neutral, optimistic, and pessimistic priors, respectively). There was a very low probability that the effect size was equal or larger than a consensus-defined minimal clinically important difference. Patients allocated to the accelerated strategy had a lower number of KRT-free days (median absolute difference of - 3.55 days [95% CrI - 6.38; - 0.48]), with a probability that the accelerated strategy was associated with more KRT-free days of 0.008. Hospital-free days were similar between strategies, with the accelerated strategy having a median absolute difference of 0.48 more hospital-free days (95% CrI - 1.87; 2.72) compared with the standard strategy and the probability that the accelerated strategy had more hospital-free days was 0.66.
Conclusions: In a Bayesian reanalysis of the STARRT-AKI trial, we found very low probability that an accelerated strategy has clinically important benefits compared with the standard strategy. Patients receiving the accelerated strategy probably have fewer days alive and KRT-free. These findings do not support the adoption of an accelerated strategy of KRT initiation.
Keywords: Acute kidney injury; Bayesian; Dialysis; Kidney-replacement therapy; Mortality; Randomized; Trial.
© 2022. The Author(s).
Conflict of interest statement
FGZ has received Grants for investigator initiated clinical trials from Bactiguard (Sweden) and Ionis Pharmaceuticals (USA), unrelated to this work. FGZ has performed statistical consulting for Bactiguard (Sweden). FGZ does not own stocks, neither has been reimbursed for travels or has received speaking fees. MO has received speaker fees and research funding from Baxter and Fresenius Medical Care. SMB has received speaker and Scientific Advisory fees and unrestricted research funding from Baxter and Scientific Advisor fees from Novartis and BioPorto. RW has received unrestricted research funding from Baxter.
Figures
References
-
- STARRT-AKI Investigators, Bagshaw SM, Wald R, et al. Timing of initiation of renal-replacement therapy in acute kidney injury. N Engl J Med. 2020;383(3):240–51. 10.1056/NEJMoa2000741. - PubMed
-
- Zarbock A, Kellum JA, Schmidt C, et al. Effect of early vs delayed initiation of renal replacement therapy on mortality in critically ill patients with acute kidney injury: the ELAIN randomized clinical trial. JAMA. 2016;315(20):2190–9. 10.1001/jama.2016.5828. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
