

How Effective Is a Late-Onset Antihypertensive Treatment? Studies with Captopril as Monotherapy and in Combination with Nifedipine in Old Spontaneously Hypertensive Rats
- PMID: 36009511
- PMCID: PMC9406136
- DOI: 10.3390/biomedicines10081964
How Effective Is a Late-Onset Antihypertensive Treatment? Studies with Captopril as Monotherapy and in Combination with Nifedipine in Old Spontaneously Hypertensive Rats
Abstract
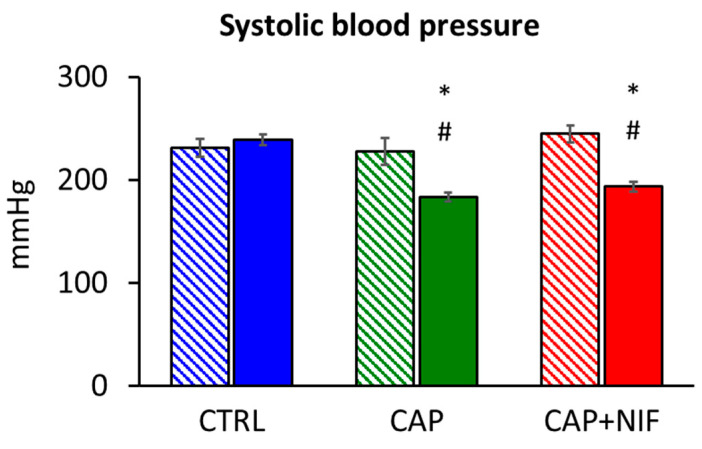
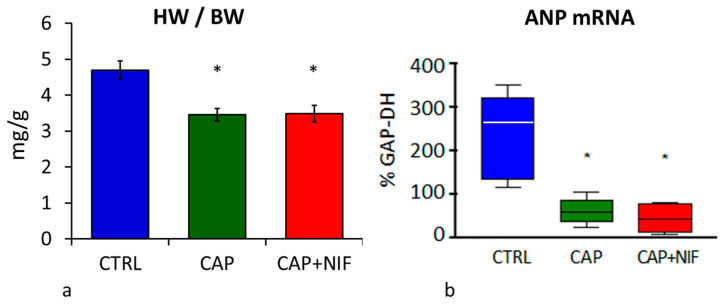
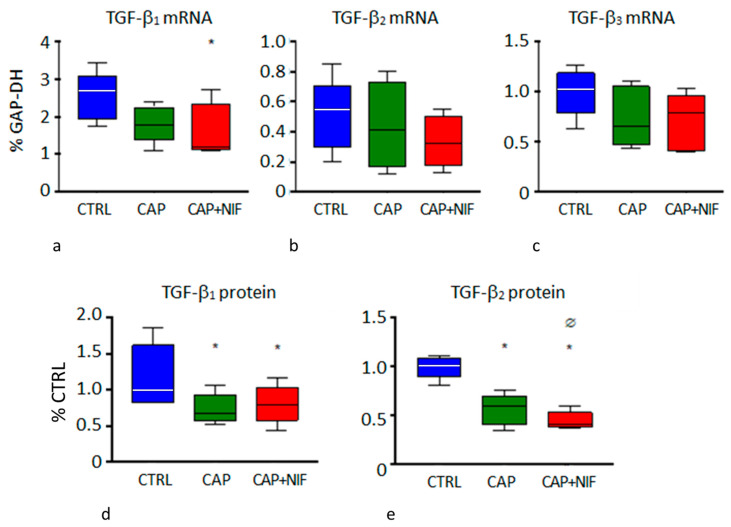
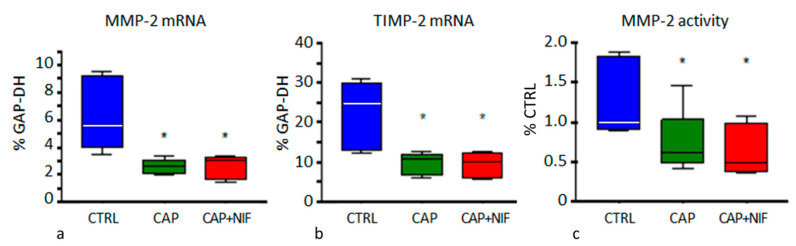
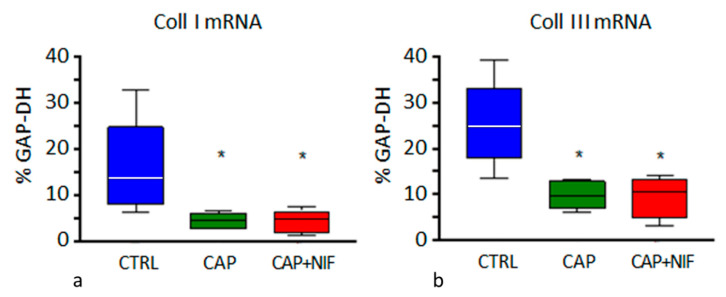
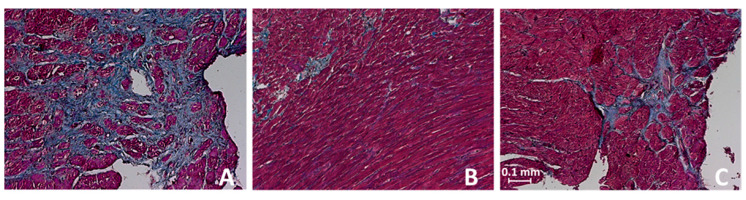
Background: A major problem in the treatment of human hypertension is the late diagnosis of hypertension and, hence, the delayed start of treatment. Very often, hypertension has existed for a long time and cardiac damage has already developed. Therefore, we tested whether late-onset antihypertensive treatment is effective in lowering blood pressure (BP) and in reducing or even preventing left ventricular hypertrophy and fibrosis. Methods: Twenty-one male 60-week-old spontaneously hypertensive rats (SHR) were included. Fourteen rats received oral treatment with captopril (CAP) either as monotherapy or combined with nifedipine (CAP + NIF) over 22 weeks. Seven untreated SHR served as controls. We examined the therapeutic effects on BP, heart weight and histological and biochemical markers of left ventricular remodeling and fibrosis. Results: At 82 weeks of age, BP was reduced in the CAP and CAP + NIF groups by 44 and 51 mmHg, respectively (p < 0.001), but not in untreated controls. Despite the late therapy start, cardiac hypertrophy and fibrosis were attenuated compared to controls. Both treatments reduced heart weight by 1.2 mg/g (25%, p = 0.001) and collagens I and III by 66% and 60%, respectively (p < 0.001), thus proving nearly equivalent cardioprotective efficacy. Conclusion: These data clearly emphasize the benefit of antihypertensive treatment in reducing BP and mitigating the development of cardiac damage even when treatment is started late in life.
Keywords: ECM markers; LV hypertrophy; antihypertensive therapy; blood pressure monitoring; cardiac fibrosis; old SHR.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
How Do Young and Old Spontaneously Hypertensive Rats Respond to Antihypertensive Therapy? Comparative Studies on the Effects of Combined Captopril and Nifedipine Treatment.Biomedicines. 2022 Nov 28;10(12):3059. doi: 10.3390/biomedicines10123059. Biomedicines. 2022. PMID: 36551815 Free PMC article.
-
Effects of late-onset and long-term captopril and nifedipine treatment in aged spontaneously hypertensive rats: Echocardiographic studies.Hypertens Res. 2015 Nov;38(11):716-22. doi: 10.1038/hr.2015.68. Epub 2015 Jul 16. Hypertens Res. 2015. PMID: 26178152
-
Antihypertensive and cardioprotective effects of different monotherapies and combination therapies in young spontaneously hypertensive rats - A pilot study.Saudi J Biol Sci. 2022 Jan;29(1):339-345. doi: 10.1016/j.sjbs.2021.08.093. Epub 2021 Sep 8. Saudi J Biol Sci. 2022. PMID: 35002427 Free PMC article.
-
Regression of myocardial fibrosis in hypertensive heart disease: diverse effects of various antihypertensive drugs.Cardiovasc Res. 2000 May;46(2):324-31. doi: 10.1016/s0008-6363(99)00432-0. Cardiovasc Res. 2000. PMID: 10773237
-
Withdrawal reveals lack of effect of prolonged antihypertensive treatment on intrinsic aortic wall stiffness in senescent spontaneously hypertensive rats.Clin Exp Pharmacol Physiol. 2002 Oct;29(10):898-904. doi: 10.1046/j.1440-1681.2002.03747.x. Clin Exp Pharmacol Physiol. 2002. PMID: 12207569
Cited by
-
How Do Young and Old Spontaneously Hypertensive Rats Respond to Antihypertensive Therapy? Comparative Studies on the Effects of Combined Captopril and Nifedipine Treatment.Biomedicines. 2022 Nov 28;10(12):3059. doi: 10.3390/biomedicines10123059. Biomedicines. 2022. PMID: 36551815 Free PMC article.
-
Angiotensin II-mediated hippocampal hypoperfusion and vascular dysfunction contribute to vascular cognitive impairment in aged hypertensive rats.Alzheimers Dement. 2024 Feb;20(2):890-903. doi: 10.1002/alz.13491. Epub 2023 Oct 10. Alzheimers Dement. 2024. PMID: 37817376 Free PMC article.
References
-
- NCD Risk Factor Collaboration (NCD-RisC) Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398:957–980. doi: 10.1016/S0140-6736(21)01330-1. - DOI - PMC - PubMed
-
- Demirci B., McKeown P.P., Bayraktutan U. Blockade of angiotensin II provides additional benefits in hypertension- and ageing-related cardiac and vascular dysfunctions beyond its blood pressure-lowering effects. J. Hypertens. 2005;23:2219–2227. doi: 10.1097/01.hjh.0000191906.03983.ee. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
