

Latency Trend Analysis as a Guide to Screening Malignancy Survivors for Second Primary Thyroid Cancer
- PMID: 36009531
- PMCID: PMC9406053
- DOI: 10.3390/biomedicines10081984
Latency Trend Analysis as a Guide to Screening Malignancy Survivors for Second Primary Thyroid Cancer
Abstract
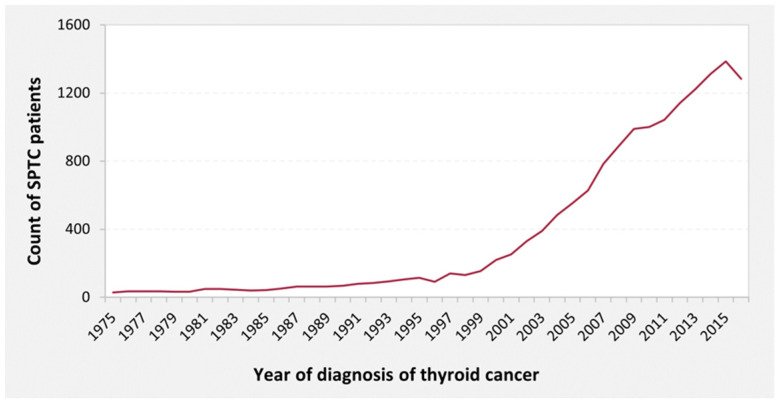
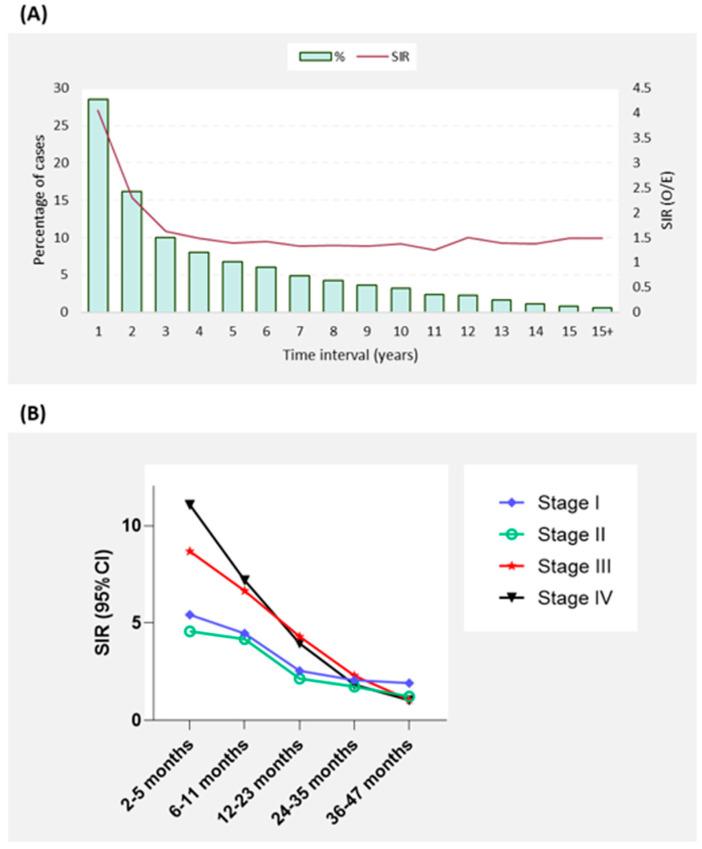
Primary cancer survivors have a higher risk of developing second primary thyroid cancer (SPTC). Patients with SPTC who survived primary malignancies, diagnosed from 1975 to 2016, were identified from the Surveillance, Epidemiology, and End Results (SEER) database (SEER 18 Registry). A total of 33,551 cancer cases were enrolled in the final analysis. Individuals with a primary malignancy were at a significant 90% increased risk of developing SPTC (SIR = 1.90, 95%CI = 1.86−1.93, p < 0.05) compared to the general population. More than half (54.7%) of SPTC diagnoses were made in the first three years after primary cancer diagnosis, and the most aggressive presentations of SPTC occurred within the first year following malignancy. A latency trend analysis identified persistent high risk for development of SPTC after diagnosis of lymphoma, leukemia, soft tissue tumors, kidney, breast, and uterine cancer; elevated 10-year risk for most cancers such as salivary gland, melanoma, stomach, lung, colon, ovarian, pancreas, prostate, and bladder; and high 5-year risk after cancers such as larynx, oral, orbit, bone, small intestine, and liver. Our latency period model identifying risk according to each type of primary cancer may aid clinicians in identifying at-risk patients to be screened for thyroid cancer and guide them in developing a surveillance plan according to the latency period attributed to a patient’s primary cancer.
Keywords: SEER; screening; second primary thyroid cancer; thyroid latency.
Conflict of interest statement
The authors declare no conflict of interest. The sponsors had no role in the design, execution, interpretation, or writing of the study.
Figures




Similar articles
-
Risk of second primary thyroid cancer in cancer survivors.Sci Rep. 2024 May 30;14(1):12478. doi: 10.1038/s41598-024-63155-z. Sci Rep. 2024. PMID: 38816510 Free PMC article.
-
Sexual disparity and the risk of second primary thyroid cancer: a paradox.Gland Surg. 2023 Apr 28;12(4):432-441. doi: 10.21037/gs-22-411. Epub 2023 Mar 28. Gland Surg. 2023. PMID: 37200932 Free PMC article.
-
Risk of subsequent primary thyroid cancer after another malignancy: latency trends in a population-based study.Ann Surg Oncol. 2012 Jun;19(6):1887-96. doi: 10.1245/s10434-011-2193-2. Epub 2012 Jan 7. Ann Surg Oncol. 2012. PMID: 22227921 Free PMC article.
-
Risk of second primary malignancies following cutaneous melanoma diagnosis: a population-based study.J Am Acad Dermatol. 2010 May;62(5):757-67. doi: 10.1016/j.jaad.2009.07.039. Epub 2010 Mar 12. J Am Acad Dermatol. 2010. PMID: 20223559
-
Radiation and Second Primary Thyroid Cancer Following Index Head and Neck Cancer.Laryngoscope. 2019 Apr;129(4):1014-1020. doi: 10.1002/lary.27467. Epub 2018 Sep 12. Laryngoscope. 2019. PMID: 30208210
Cited by
-
Risk of second primary thyroid cancer in cancer survivors.Sci Rep. 2024 May 30;14(1):12478. doi: 10.1038/s41598-024-63155-z. Sci Rep. 2024. PMID: 38816510 Free PMC article.
-
Sexual disparity and the risk of second primary thyroid cancer: a paradox.Gland Surg. 2023 Apr 28;12(4):432-441. doi: 10.21037/gs-22-411. Epub 2023 Mar 28. Gland Surg. 2023. PMID: 37200932 Free PMC article.
-
Investigating additional malignancy rates and prognostic factors in multiple myeloma patients: a Surveillance, Epidemiology, and End Results (SEER) database retrospective cohort study.Transl Cancer Res. 2025 Apr 30;14(4):2192-2206. doi: 10.21037/tcr-24-1721. Epub 2025 Apr 14. Transl Cancer Res. 2025. PMID: 40386261 Free PMC article.
-
Ultraviolet Light Exposure Decreases Thyroid Cancer Risk: A National Perspective.Biomedicines. 2022 Oct 1;10(10):2452. doi: 10.3390/biomedicines10102452. Biomedicines. 2022. PMID: 36289713 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
