

The Ratio of the Size of the Abdominal Aortic Aneurysm to That of the Unchanged Aorta as a Risk Factor for Its Rupture
- PMID: 36009543
- PMCID: PMC9405575
- DOI: 10.3390/biomedicines10081997
The Ratio of the Size of the Abdominal Aortic Aneurysm to That of the Unchanged Aorta as a Risk Factor for Its Rupture
Abstract
Background: A ruptured abdominal aortic aneurysm is a severe condition associated with high mortality. Currently, the most important criterion used to estimate the risk of its rupture is the size of the aneurysm, but due to patients' anatomical variability, many aneurysms have a high risk of rupture with a small aneurysm size. We asked ourselves whether individual differences in anatomy could be taken into account when assessing the risk of rupture.
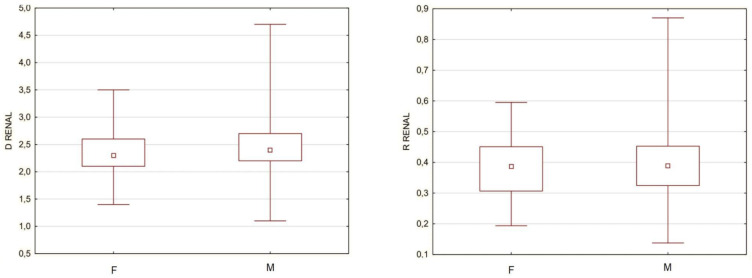
Methods: Based on the CT scan image, aneurysm and normal aorta diameters were collected from 186 individuals and compared in patients with ruptured and unruptured aneurysms. To take into account anatomical differences between patients, diameter ratios were calculated by dividing the aneurysm diameter by the diameter of the normal aorta at various heights, and then further comparisons were made.
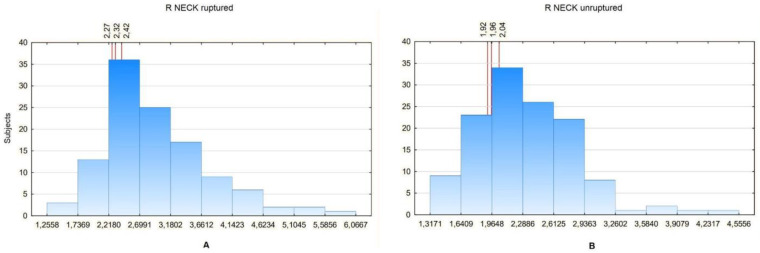
Results: It was found that the calculated ratios differ between patients with ruptured and unruptured aneurysms. This observation is also present in patients with small aneurysms, with its maximal size below the level that indicates the need for surgical treatment. For small aneurysms, the ratios help us to estimate the risk of rupture better than the maximum sac size (AUC: 0.783 vs. 0.650).
Conclusions: The calculated ratios appear to be a valuable feature to indicate which of the small aneurysms have a high risk of rupture. The obtained results suggest the need for further confirmation of their usefulness in subsequent groups of patients.
Keywords: aneurysm rupture risk assessment; aneurysm rupture risk factors; ruptured abdominal aortic aneurysm.
Conflict of interest statement
The authors declare no conflict of interest.
Figures








References
-
- Raux M., Marzelle J., Kobeiter H., Dhonneur G., Allaire E., Cochennec F., Becquemin J.-P., Desgranges P. Endovascular balloon occlusion is associated with reduced intraoperative mortality of unstable patients with ruptured abdominal aortic aneurysm but fails to improve other outcomes. J. Vasc. Surg. 2015;61:304–308. doi: 10.1016/j.jvs.2014.07.098. - DOI - PubMed
LinkOut - more resources
Full Text Sources
