

A Proof of Concept of the Usefulness of a TDM-Guided Strategy for Optimizing Pharmacokinetic/Pharmacodynamic Target of Continuous Infusion Ampicillin-Based Regimens in a Case Series of Patients with Enterococcal Bloodstream Infections and/or Endocarditis
- PMID: 36009906
- PMCID: PMC9404876
- DOI: 10.3390/antibiotics11081037
A Proof of Concept of the Usefulness of a TDM-Guided Strategy for Optimizing Pharmacokinetic/Pharmacodynamic Target of Continuous Infusion Ampicillin-Based Regimens in a Case Series of Patients with Enterococcal Bloodstream Infections and/or Endocarditis
Abstract
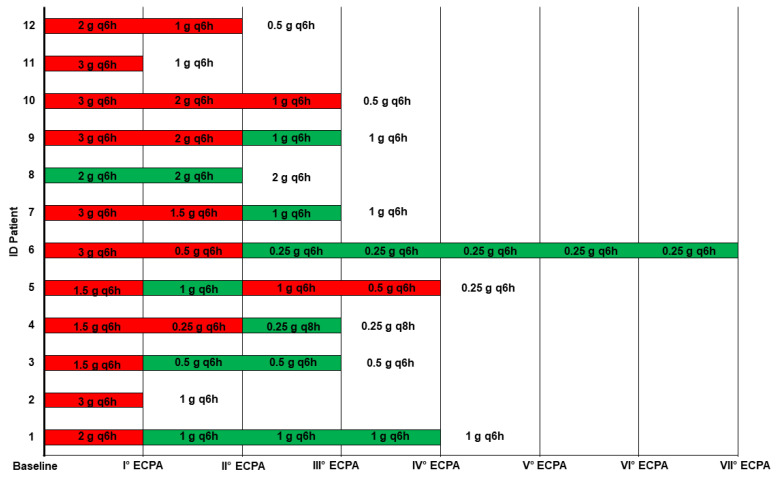
(1) Objective: To describe the usefulness of a real-time therapeutic drug monitoring (TDM)-based strategy for optimizing pharmacokinetic/pharmacodynamic (PK/PD) target attainment of continuous infusion (CI) ampicillin-based regimens in a case series of patients affected by suspected or documented enterococcal bloodstream infections (BSIs) and/or infective endocarditis (IE). (2) Methods: Patients treated with CI ampicillin-based regimens for documented or suspected enterococcal BSI/IE who underwent real-time therapeutic drug monitoring (TDM)-based expert clinical pharmacological advice (ECPA) between June 2021 and May 2022 were retrospectively assessed. Ampicillin concentrations were determined at steady state, and the free fraction (fCss) was calculated according to a plasma protein binding of 20%. The fCss/MIC ratio was selected as the PD parameter for ampicillin efficacy and was defined as optimal for values between 4 and 8. The requirement for TDM-guided ampicillin dosing adjustments was assessed. (3) Results: Data for 12 patients with documented (n = 10) or suspected (n = 2) enterococcal infections (7 with BSIs and 5 with IE) were retrieved. The ampicillin PK/PD target was optimal over time in all of the 10 documented infections. None of the enterococcal BSIs persisted. Following the first real-time TDM-based ECPA, ampicillin dosage was decreased by >50% in 11 out of 12 patients (91.7%). (4) Conclusions: CI may be helpful in attaining aggressive ampicillin PK/PD targets in patients affected by enterococcal BSIs and/or IE. Administration of CI ampicillin after loading coupled with real-time TDM-based ECPA could be a valuable strategy for managing enterococcal infections.
Keywords: Enterococcus faecalis; TDM-guided dosing adjustment; ampicillin; bloodstream infections; continuous infusion; endocarditis.
Conflict of interest statement
MiGa has received personal fees from Angelini and Shionogi, outside the submitted work. PV has served as a consultant for bioMérieux, Gilead, Merck Sharp and Dohme, Nabriva, Nordic Pharma, Pfizer, Thermo-Fisher, and Venatorx, and received payment for serving on the speaker’s bureaus for Correvio, Gilead, Merck Sharp and Dohme, Nordic Pharma, and Pfizer, outside the submitted work. FP has participated in speaker bureaus for Angelini, Basilea Pharmaceutica, Gilead, Hikma, Merck Sharp and Dohme, Nordic Pharma, Pfizer, and Sanofi Aventis, and served on advisory boards for Angelini, Basilea Pharmaceutica, Gilead, Hikma, Merck Sharp and Dohme, Nordic Pharma, Novartis, Pfizer, and Shionogi, outside the submitted work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Habib G., Lancellotti P., Antunes M.J., Bongiorni M.G., Casalta J.-P., Del Zotti F., Dulgheru R., El Khoury G., Erba P.A., Iung B., et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM) Eur. Heart J. 2015;36:3075–3128. doi: 10.1093/eurheartj/ehv319. - DOI - PubMed
-
- Fernández-Hidalgo N., Almirante B., Gavaldà J., Gurgui M., Peña C., de Alarcón A., Ruiz J., Vilacosta I., Montejo M., Vallejo N., et al. Ampicillin Plus Ceftriaxone Is as Effective as Ampicillin Plus Gentamicin for Treating Enterococcus faecalis Infective Endocarditis. Clin. Infect. Dis. 2013;56:1261–1268. doi: 10.1093/cid/cit052. - DOI - PubMed
-
- Gavaldà J., Len O., Miró J.M., Muñoz P., Montejo M., Alarcón A., de la Torre-Cisneros J., Peña C., Martínez-Lacasa X., Sarria C., et al. Brief Communication: Treatment of Enterococcus Faecalis Endocarditis with Ampicillin plus Ceftriaxone. Ann. Intern. Med. 2007;146:574–579. doi: 10.7326/0003-4819-146-8-200704170-00008. - DOI - PubMed
LinkOut - more resources
Full Text Sources
