

MRI Evolution of a Patient with Viral Tick-Borne Encephalitis and Polymorphic Seizures
- PMID: 36010239
- PMCID: PMC9406907
- DOI: 10.3390/diagnostics12081888
MRI Evolution of a Patient with Viral Tick-Borne Encephalitis and Polymorphic Seizures
Abstract
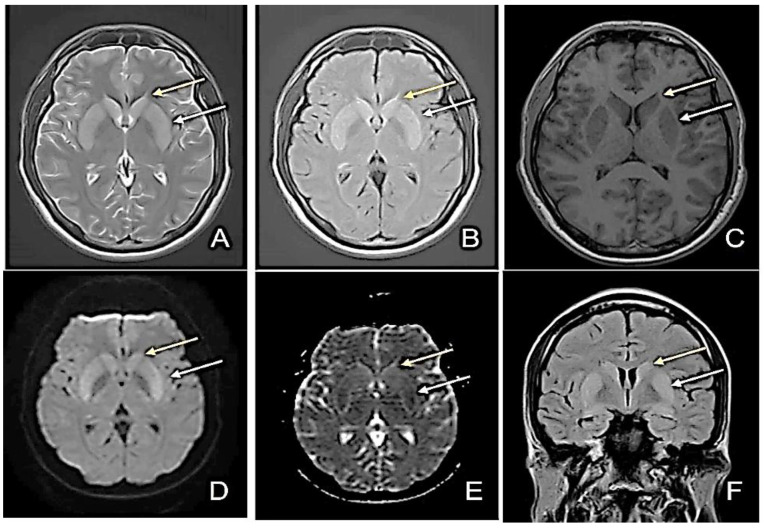
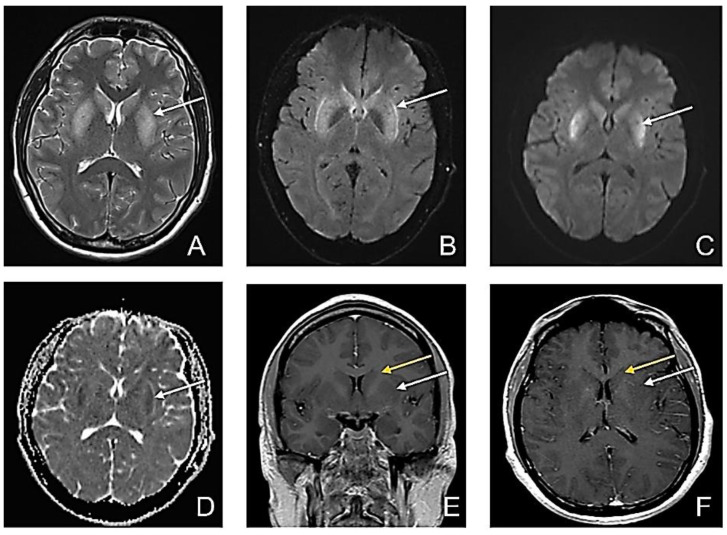
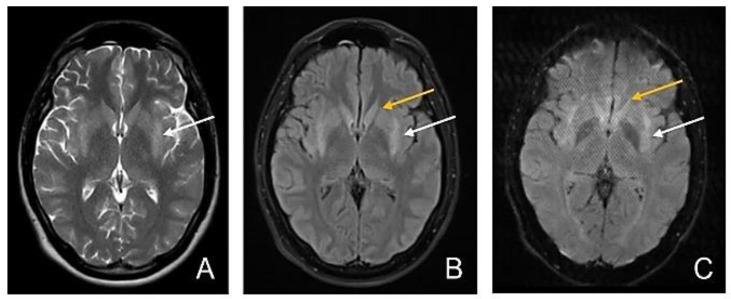
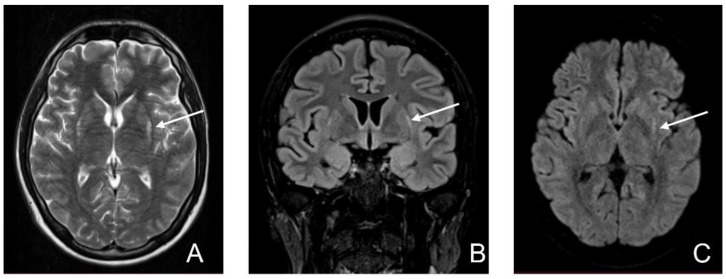
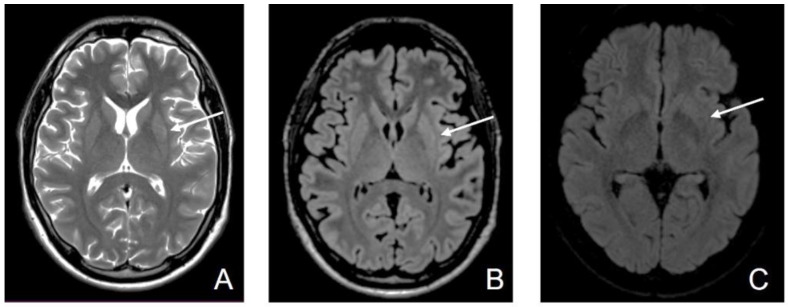
Some neurotropic viruses induce specific lesions in the deep structures, such as basal ganglia and thalamus. These anatomical structures play an important role in initiating and maintaining different types of epileptic seizures. We present the case of a 25-year-old male, transferred to our clinic one week after the onset of the symptomatology, with a recent history of traveling to Turkey and Egypt. At the moment of his hospital admission, his symptoms included altered consciousness, agitation, and seizures. Shortly after, his state worsened, requiring intubation. Viral tick-borne encephalitis diagnoses were favored by the CSF (cerebrospinal fluid) analysis, EEG (Electroencephalography), MRI (magnetic resonance imaging) images presenting symmetric hyper signal in the basal ganglia, and IgM antibodies for anti-tick-borne encephalitis. These lesions persisted for several weeks, and the patient's seizures were polymorphic, originally generalized onset motor, generalized onset non-motor, and focal myoclonic. The patient achieved his independence, seizures decreasing both in intensity and frequency; the MRI images became almost normal. The reduction in antiepileptic doses was not followed by seizure recurrence.
Keywords: CSF; EEG; MRI; basal ganglia; flavivirus; imaging; polymorphic seizures; tick-borne encephalitis (TBE); tick-borne encephalitis virus (TBEV).
Conflict of interest statement
Sirbu CA has received speaker honoraria, consulting fees, travel fees, and research and educational grants from Bayer, Novartis, Merck, Schering, Ever Pharma, Roche, and Teva. Not applicable to the rest of the authors.
Figures
References
-
- Ruzek D., Županc T.A., Borde J., Chrdle A., Eyer L., Karganova G., Kholodilov I., Knap N., Kozlovskaya L., Matveev A., et al. Tick-borne encephalitis in Europe and Russia: Review of pathogenesis, clinical features, therapy, and vaccines. Antivir. Res. 2019;164:23–51. doi: 10.1016/j.antiviral.2019.01.014. - DOI - PubMed
LinkOut - more resources
Full Text Sources
