

The Role of CT in the Staging and Follow-Up of Testicular Tumors: Baseline, Recurrence and Pitfalls
- PMID: 36010958
- PMCID: PMC9406011
- DOI: 10.3390/cancers14163965
The Role of CT in the Staging and Follow-Up of Testicular Tumors: Baseline, Recurrence and Pitfalls
Abstract
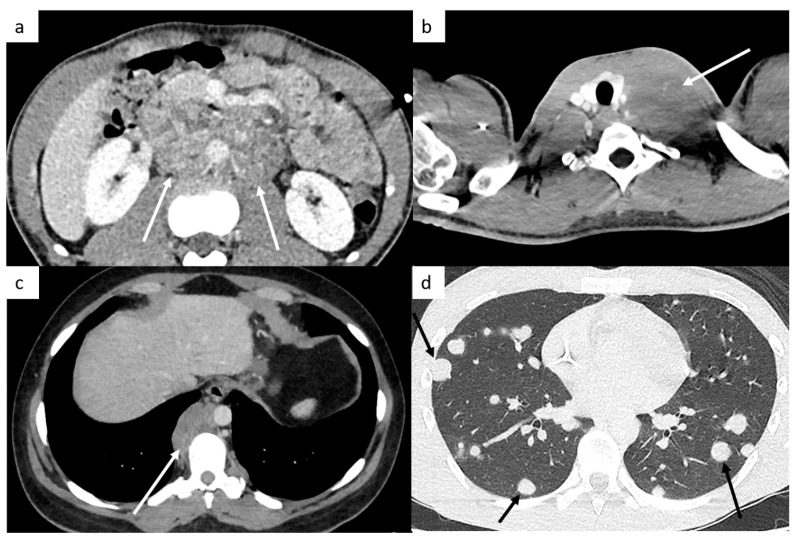
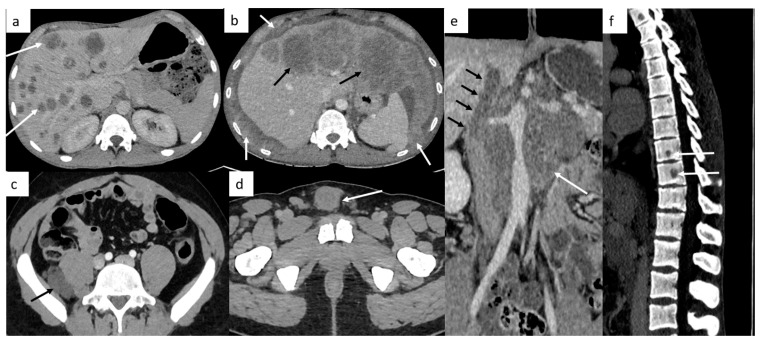
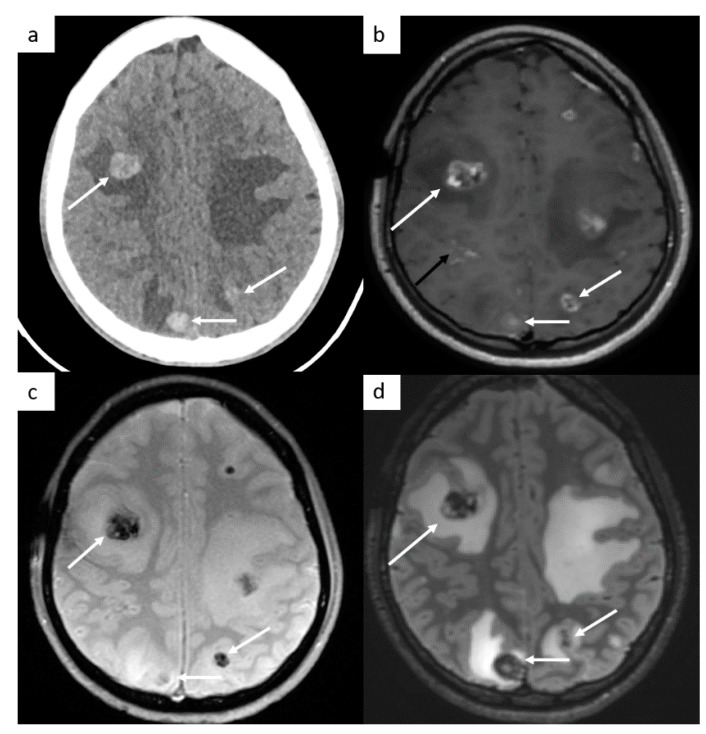
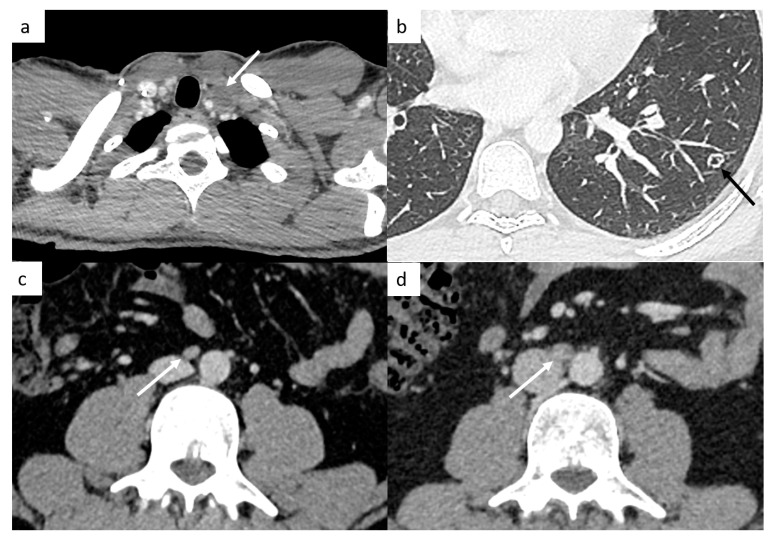
Ultrasound imaging of the testis represents the standard-of-care initial imaging for the diagnosis of TGCT, whereas computed tomography (CT) plays an integral role in the initial accurate disease staging (organ-confined, regional lymph nodes, or sites of distant metastases), in monitoring the response to therapy in patients who initially present with non-confined disease, in planning surgical approaches for residual masses, in conducting follow-up surveillance and in determining the extent of recurrence in patients who relapse after treatment completion. CT imaging has also an important place in diagnosing complications of treatments. The aims of this article are to review these different roles of CT in primary TGCT and focus on different pitfalls that radiologists need to be aware of.
Keywords: computed tomography (CT); germ cells tumors (GCT); oncologic diagnostic imaging; retroperitoneal masses; seminomatous and nonseminomatous GCT; testicular cancer (TC).
Conflict of interest statement
Karim Fizazi: Participation on advisory boards and talks for: Amgen, Astellas, Astrazeneca, Bayer, Clovis, Daiichi Sankyo, Janssen, MSD, Novartis/AAA, Pfizer, Sanofi. Honoraria go to Gustave Roussy and my institution. Participation on advisory boards with personal honorarium for CureVac and Orion. Other authors declare no conflict of interest.
Figures
References
-
- World Cancer Research Fund Worldwide Cancer Data: Global Cancer Statistics for the Most Common Cancers. [(accessed on 21 January 2022)]. Available online: https://www.wcrf.org/dietandcancer/cancer-trends/worldwide-cancer-data.
Publication types
LinkOut - more resources
Full Text Sources
