

Proposing a Scientific and Technological Approach to the Summaries of Clinical Issues of Inpatient Elderly with Delirium: A Viewpoint
- PMID: 36011191
- PMCID: PMC9408148
- DOI: 10.3390/healthcare10081534
Proposing a Scientific and Technological Approach to the Summaries of Clinical Issues of Inpatient Elderly with Delirium: A Viewpoint
Abstract
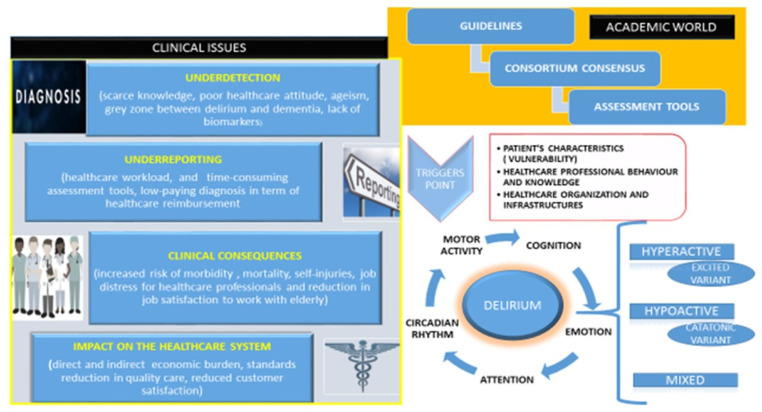
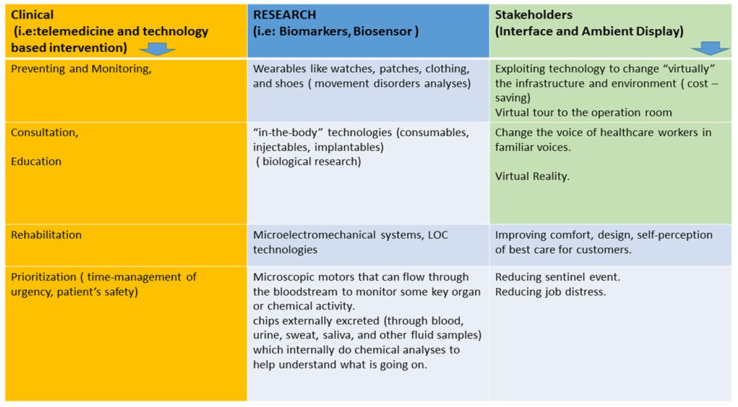
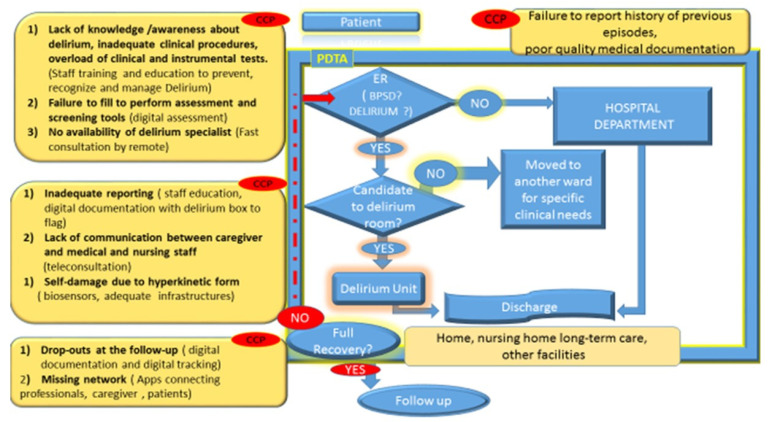
Background/rationale: Despite mounting evidence about delirium, this complex geriatric syndrome is still not well managed in clinical contexts. The aging population creates a very demanding area for innovation and technology in healthcare. For instance, an outline of an aging-friendly healthcare environment and clear guidance for technology-supported improvements for people at delirium risk are lacking. Objective: We aimed to foster debate about the importance of technical support in optimizing healthcare professional practice and improving the outcomes for inpatients' at delirium risk. We focused on critical clinical points in the field of delirium worthy of being addressed by a multidisciplinary approach. Methods: Starting from a consensus workshop sponsored by the Management Perfectioning Course based at the Marco Biagi Foundation (Modena, Italy) about clinical issues related to delirium management still not addressed in our healthcare organizations, we developed a requirements' analysis among the representatives of different disciplines and tried to formulate how technology could support the summaries of the clinical issues. We analyzed the national and international panorama by a PubMed consultation of articles with the following keywords in advanced research: "delirium", "delirium management", "technology in healthcare", and "elderly population". Results: Despite international recommendations, delirium remains underdiagnosed, underdetected, underreported, and mismanaged in the acute hospital, increasing healthcare costs, healthcare professionals' job distress, and poor clinical outcomes. Discussion: Although all healthcare professionals recognize delirium as a severe and potentially preventable source of morbidity and mortality for hospitalized older people, it receives insufficient attention in resource allocation and multidisciplinary research. We synthesized how tech-based tools could offer potential solutions to the critical clinical points in delirium management.
Keywords: delirium; disease management; healthcare; patient care management; technology; telemedicine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Delirium in older hospitalized patients-signs and actions: a retrospective patient record review.BMC Geriatr. 2018 Feb 6;18(1):43. doi: 10.1186/s12877-018-0731-5. BMC Geriatr. 2018. PMID: 29409468 Free PMC article.
-
How has the impact of 'care pathway technologies' on service integration in stroke care been measured and what is the strength of the evidence to support their effectiveness in this respect?Int J Evid Based Healthc. 2008 Mar;6(1):78-110. doi: 10.1111/j.1744-1609.2007.00098.x. Int J Evid Based Healthc. 2008. PMID: 21631815
-
Toward the realization of a better aged society: messages from gerontology and geriatrics.Geriatr Gerontol Int. 2012 Jan;12(1):16-22. doi: 10.1111/j.1447-0594.2011.00776.x. Geriatr Gerontol Int. 2012. PMID: 22188494 Review.
-
Delirium in the elderly: Current problems with increasing geriatric age.Indian J Med Res. 2015 Dec;142(6):655-62. doi: 10.4103/0971-5916.174546. Indian J Med Res. 2015. PMID: 26831414 Free PMC article. Review.
Cited by
-
Delirium Diagnosis, Complication Recognition, and Treatment Knowledge among Nurses in an Italian Local Hospital: A Cross-Sectional Study.Nurs Rep. 2024 Mar 27;14(2):767-776. doi: 10.3390/nursrep14020059. Nurs Rep. 2024. PMID: 38651471 Free PMC article.
-
Factors involved in the development of hospital-acquired conditions in older patients in acute care settings: a scoping review.BMC Health Serv Res. 2025 Jan 29;25(1):174. doi: 10.1186/s12913-025-12318-3. BMC Health Serv Res. 2025. PMID: 39881323 Free PMC article.
References
-
- Rogers J.P., Chesney E., Oliver D., Pollak T.A., McGuire P., Fusar-Poli P., Zandi M.S., Lewis G., David A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. 2020;7:611–627. doi: 10.1016/S2215-0366(20)30203-0. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
