

Pancreatic Incidentaloma
- PMID: 36012893
- PMCID: PMC9409921
- DOI: 10.3390/jcm11164648
Pancreatic Incidentaloma
Abstract
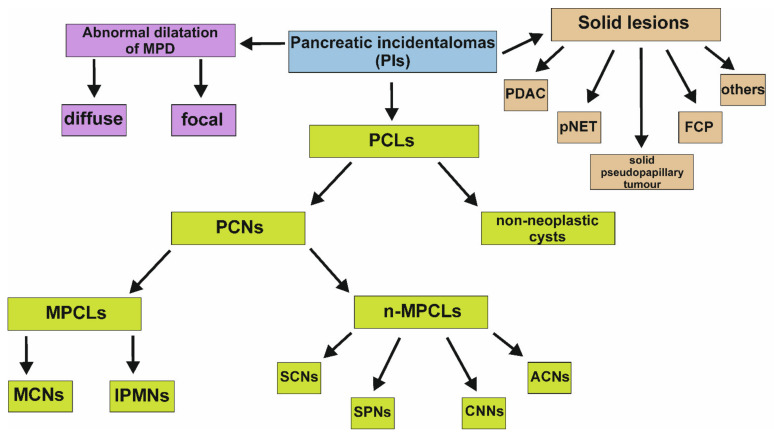
Pancreatic incidentalomas (PIs) represent a clinical entity increasingly recognized due to advances in and easier access to imaging techniques. By definition, PIs should be detected during abdominal imaging performed for indications other than a pancreatic disease. They range from small cysts to invasive cancer. The incidental diagnosis of pancreatic cancer can contribute to early diagnosis and treatment. On the other hand, inadequate management of PIs may result in overtreatment and unneeded morbidity. Therefore, there is a strong need to evaluate the nature and clinical features of individual PIs. In this review, we summarize the major characteristics related to PIs and present suggestions for their management.
Keywords: cysts; early detection; incidentaloma; neoplasm; pancreas; pancreatic cancer; pancreatic tumor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Herrera M.F., Pantoja J.P., Salazar M.S., Velázquez-Fernández D. Endocrine Surgery. Springer; London, UK: 2009. Pancreatic Incidentaloma; pp. 541–552. - DOI
-
- Karatzas T., Dimitroulis D., Charalampoudis P., Misiakos E.P., Vasileiadis I., Kouraklis G. Management of cystic and solid pancreatic incidentalomas: A review analysis. JBUON. 2013;18:17–24. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
