

COVID-19-Related ARDS: Key Mechanistic Features and Treatments
- PMID: 36013135
- PMCID: PMC9410336
- DOI: 10.3390/jcm11164896
COVID-19-Related ARDS: Key Mechanistic Features and Treatments
Abstract
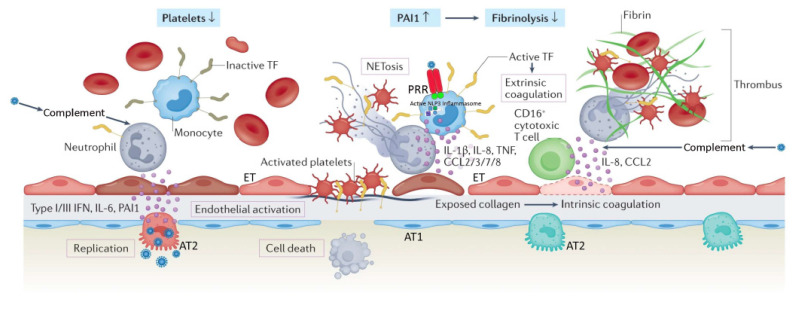
Acute respiratory distress syndrome (ARDS) is a heterogeneous syndrome historically characterized by the presence of severe hypoxemia, high-permeability pulmonary edema manifesting as diffuse alveolar infiltrate on chest radiograph, and reduced compliance of the integrated respiratory system as a result of widespread compressive atelectasis and fluid-filled alveoli. Coronavirus disease 19 (COVID-19)-associated ARDS (C-ARDS) is a novel etiology caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that may present with distinct clinical features as a result of the viral pathobiology unique to SARS-CoV-2. In particular, severe injury to the pulmonary vascular endothelium, accompanied by the presence of diffuse microthrombi in the pulmonary microcirculation, can lead to a clinical presentation in which the severity of impaired gas exchange becomes uncoupled from lung capacity and respiratory mechanics. The purpose of this review is to highlight the key mechanistic features of C-ARDS and to discuss the implications these features have on its treatment. In some patients with C-ARDS, rigid adherence to guidelines derived from clinical trials in the pre-COVID era may not be appropriate.
Keywords: COVID-19; SARS-CoV-2; acute respiratory distress syndrome; mechanical ventilation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Thille A.W., Esteban A., Fernandez-Segoviano P., Rodriguez J.M., Aramburu J.A., Penuelas O., Cortes-Puch I., Cardinal-Fernandez P., Lorente J.A., Frutos-Vivar F. Comparison of the Berlin definition for acute respiratory distress syndrome with autopsy. Am. J. Respir. Crit. Care Med. 2013;187:761–767. doi: 10.1164/rccm.201211-1981OC. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
