

Measuring Indirect Radiation-Induced Perfusion Change in Fed Vasculature Using Dynamic Contrast CT
- PMID: 36013203
- PMCID: PMC9410208
- DOI: 10.3390/jpm12081254
Measuring Indirect Radiation-Induced Perfusion Change in Fed Vasculature Using Dynamic Contrast CT
Abstract
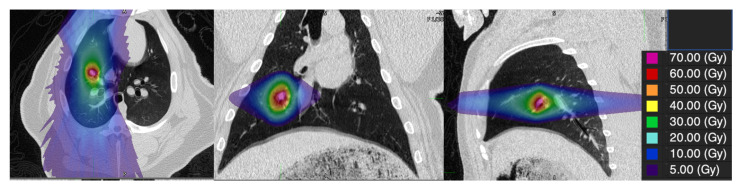
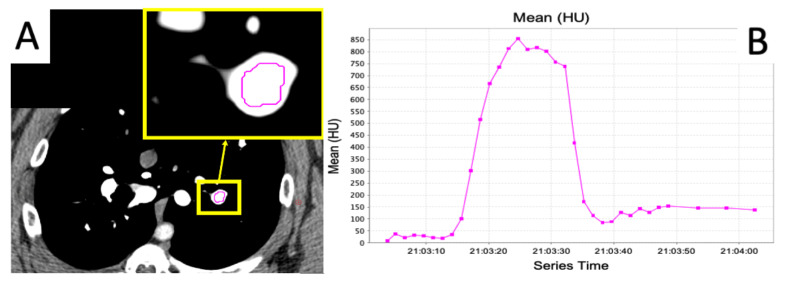
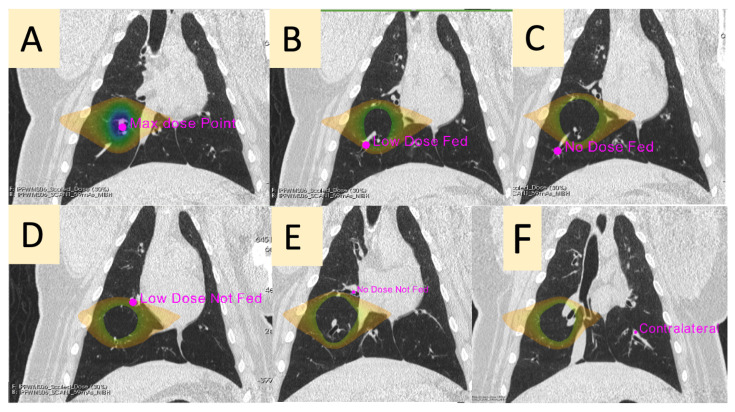
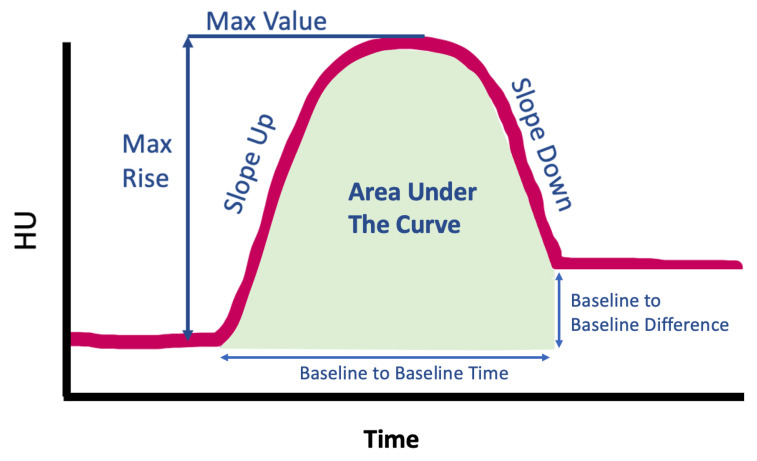
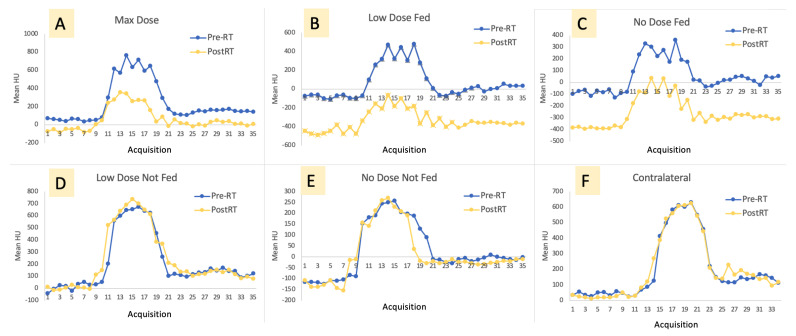
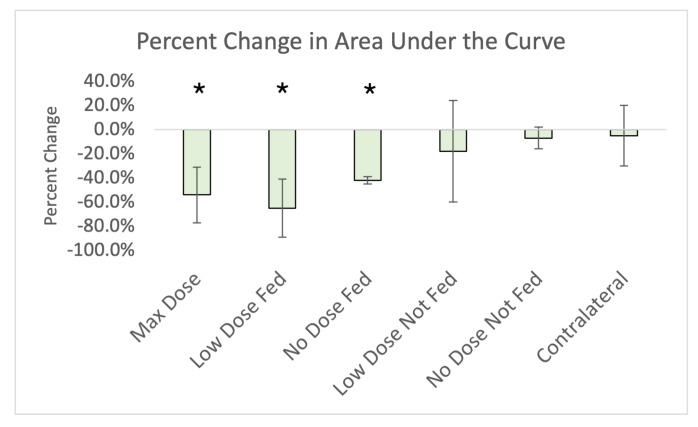
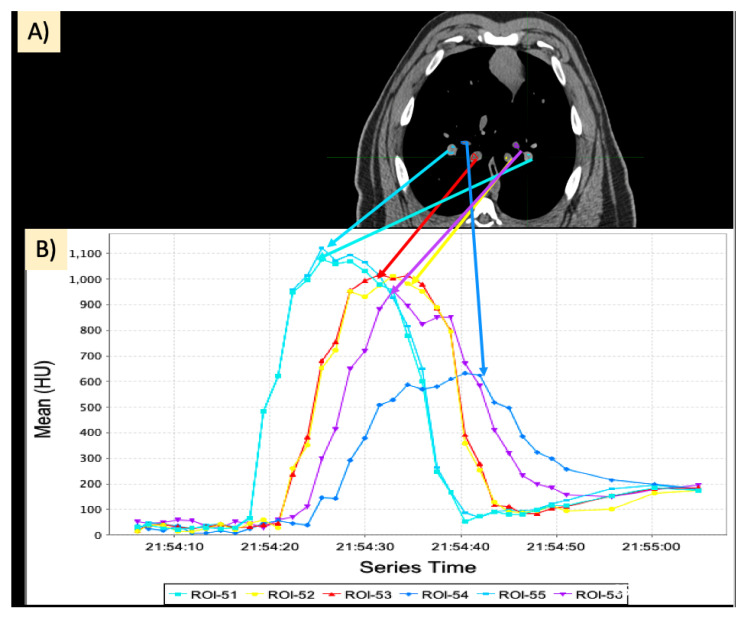
Recent functional lung imaging studies have presented evidence of an “indirect effect” on perfusion damage, where regions that are unirradiated or lowly irradiated but that are supplied by highly irradiated regions observe perfusion damage post-radiation therapy (RT). The purpose of this work was to investigate this effect using a contrast-enhanced dynamic CT protocol to measure perfusion change in five novel swine subjects. A cohort of five Wisconsin Miniature Swine (WMS) were given a research course of 60 Gy in five fractions delivered locally to a vessel in the lung using an Accuray Radixact tomotherapy system with Synchrony motion tracking to increase delivery accuracy. Imaging was performed prior to delivering RT and 3 months post-RT to yield a 28−36 frame image series showing contrast flowing in and out of the vasculature. Using MIM software, contours were placed in six vessels on each animal to yield a contrast flow curve for each vessel. The contours were placed as follows: one at the point of max dose, one low-irradiated (5−20 Gy) branching from the max dose vessel, one low-irradiated (5−20 Gy) not branching from the max dose vessel, one unirradiated (<5 Gy) branching from the max dose vessel, one unirradiated (<5 Gy) not branching from the max dose vessel, and one in the contralateral lung. Seven measurements (baseline-to-baseline time and difference, slope up and down, max rise and value, and area under the curve) were acquired for each vessel’s contrast flow curve in each subject. Paired Student t-tests showed statistically significant (p < 0.05) reductions in the area under the curve in the max dose, and both fed contours indicating an overall reduction in contrast in these regions. Additionally, there were statistically significant reductions observed when comparing pre- and post-RT in slope up and down in the max dose, low-dose fed, and no-dose fed contours but not the low-dose not-fed, no-dose not-fed, or contralateral contours. These findings suggest an indirect damage effect where irradiation of the vasculature causes a reduction in perfusion in irradiated regions as well as regions fed by the irradiated vasculature.
Keywords: functional avoidance; lung SBRT; perfusion; post-RT toxicity; swine model.
Conflict of interest statement
J.M.R. is a shareholder in VIDA Diagnostics, Inc.; G.E.C. receives licensing fees from VIDA Diagnostics, Inc.; and J.E.B. has ownership interest in MR Guidance, LLC.
Figures
References
-
- American Cancer Society . 2022-Cancer-Facts-and-Figures. American Cancer Society; Atlanta, GA, USA: 2022.
-
- Bradley J.D., Paulus R., Komaki R., Masters G., Blumenschein G., Schild S., Bogart J., Hu C., Forster K., Magliocco A., et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015;16:187–199. doi: 10.1016/S1470-2045(14)71207-0. - DOI - PMC - PubMed
-
- Patton T.J., Bayouth J.E., Bednarz B.P., Fain S.B., Reinhardt J.M., Smilowitz J. Quantifying and Modeling Radiation Therapy-Induced Ventilation Changes and Investigating the Robustness of 4DCT-Based Functional Avoidance. The University of Wisconsin-Madison; Madison, WI, USA: 2018. Technical Report.
Grants and funding
LinkOut - more resources
Full Text Sources
