

Type 1A Endoleak after TEVAR in the Aortic Arch: A Review of the Literature
- PMID: 36013228
- PMCID: PMC9410239
- DOI: 10.3390/jpm12081279
Type 1A Endoleak after TEVAR in the Aortic Arch: A Review of the Literature
Abstract
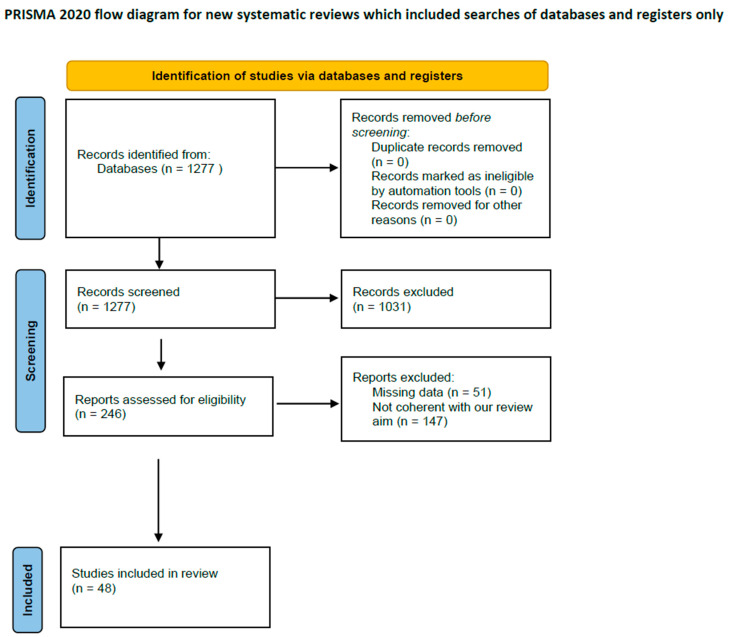
Aortic arch repair is a challenging intervention. Open surgical repair is still considered the gold standard, but in high-risk patients, it is not always a reasonable option, making endovascular approaches an enticing, when not the only available, alternative for treatment. The strategies more commonly adopted are surgical supra-aortic trunk (SAT) rerouting followed by deployment of a standard thoracic endoprosthesis, chimney techniques, custom-made scalloped, fenestrated, and branched devices, and in situ or physician-modified fenestrations. If we excluded techniques involving SAT rerouting where the arch anatomy is surgically modified in order to make deployment in the aortic arch of a standard thoracic endoprosthesis possible, in the other techniques, one or more SATs are incorporated in the thoracic endoprosthesis. In these cases, no matter what solution is adopted, because of the morphology of the aorta at this level, achieving an ideal sealing is extremely difficult, and endovascular treatments of the arch are burdened by an increased risk of type IA endoleaks. PubMed, EMBASE, and Cochrane Library were searched. We identified 1277 records. After reading titles, abstracts, and full texts, we excluded 1231 records. Exclusion criteria were low-quality evidence, abstracts, case reports, conference presentations, reviews, editorials, and expert opinions. A total of 48 studies were included, for a total of 3114 patients. A type IA endoleak occurred in 248 patients (7.7%) with a mean incidence of 18.8% in chimney procedures, 4.8% and 3%, respectively, in fenestrated and branched devices, and 2.2% in in situ fenestration. We excluded from our analysis scalloped technology that is used when the target vessel originates from a healthy landing zone and represents a different anatomical setting. Type IA endoleaks are a concern with all types of endovascular aortic arch repair, and they can compromise the outcomes of the procedure. The rate of type IA endoleaks appears to be significantly higher in chimney procedures. In order to maximize sealing, whenever possible, endovascular repair of the arch should be achieved with custom-made fenestrated devices. However, chimney configurations are still a valuable solution particularly in the emergency setting, although in such a procedure, to guarantee accurate postoperative management and follow-up, an imaging protocol could be useful.
Keywords: TEVAR; aortic arch; branched graft; chimney; endoleak; fenestrated graft; in situ fenestration.
Conflict of interest statement
Both Yamume Tshomba and Giovanni Tinelli have agreements with Terumo Aortic and Medtronic.
Figures

References
-
- Liberati A., Altman D.G., Tetzlaff J., Mulrow C., Gotzsche P.C., Ioannidis J.P.A., Clarke M., Devereaux P.J., Kleijnen J., Moher D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ (Clin. Res. Ed.) 2009;339:b2700. doi: 10.1136/bmj.b2700. - DOI - PMC - PubMed
-
- Ahmad W., Liakopoulos O.J., Mylonas S., Wegner M., Brunkwall J., Dorweiler B. Long-Term Outcomes after Thoracic Endovascular Aortic Repair Using Chimney Grafts for Aortic Arch Pathologies: 10 Years of Single-Center Experience. Ann. Vasc. Surg. 2021;72:400–408. doi: 10.1016/j.avsg.2020.08.129. - DOI - PubMed
-
- Bosiers M.J., Donas K.P., Mangialardi N., Torsello G., Riambau V., Criado F.J., Veith F.J., Ronchey S., Fazzini S., Lachat M. European Multicenter Registry for the Performance of the Chimney/Snorkel Technique in the Treatment of Aortic Arch Pathologic Conditions. Ann. Thorac. Surg. 2016;101:2224–2230. doi: 10.1016/j.athoracsur.2015.10.112. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
