

Plaster Casts vs. Intraoral Scans: Do Different Methods of Determining the Final Occlusion Affect the Simulated Outcome in Orthognathic Surgery?
- PMID: 36013237
- PMCID: PMC9409745
- DOI: 10.3390/jpm12081288
Plaster Casts vs. Intraoral Scans: Do Different Methods of Determining the Final Occlusion Affect the Simulated Outcome in Orthognathic Surgery?
Abstract
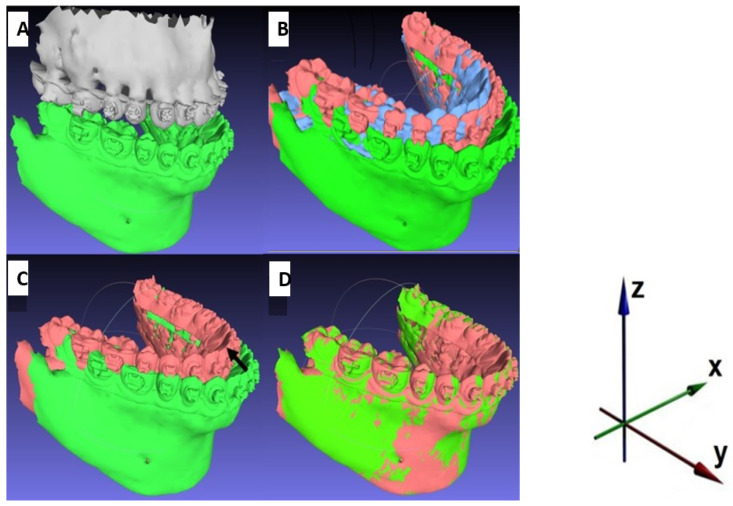
A virtual occlusal adjustment in orthognathic surgery has many advantages; however, the haptic information offered by plaster casts is missing when using intraoral scans. Feeling the interferences may be helpful in defining the best possible occlusion. Whether the use of a virtual occlusal adjustment instead of the conventional approach has a significant effect on the postsurgical position of the jaws is a question that remains unanswered. This study compares a virtual method to the conventional method of defining the final occlusion. Twenty-five orthognathic patients were included. Bimaxillary and single-jaw orthognathic surgery (mandible only) was simulated. The two methods were compared regarding discrepancies in the simulated postsurgical position of the mandible, measured three-dimensionally using MeshLab (MeshLab 2020.12 3D). An analysis using SPSS revealed no significant differences between the tested methods (p-values: 0.580 to 0.713). The mean absolute discrepancies ranged from 0.14 mm to 0.72 mm, laying within the scope of the clinically acceptable inaccuracies of an osteosynthesis in orthognathic surgery. The lack of haptic information in virtual planning had no relevant influence on the definition of the final occlusion and the simulated postsurgical outcome. However, in individual cases, plaster models might still be helpful in finding the adequate occlusion, especially in the sagittal dimension and in cases of patients with an anterior open bite, but this remains to be tested.
Keywords: digital surgery; intraoral scans; orthodontics; orthognathic surgery; virtual occlusion.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Canto G.D.L., Pacheco-Pereira C., Lagravere M.O., Flores-Mir C., Major P.W. Intra-arch dimensional measurement validity of laser-scanned digital dental models compared with the original plaster models: A systematic review. Orthod. Craniofacial Res. 2015;18:65–76. doi: 10.1111/ocr.12068. - DOI - PubMed
LinkOut - more resources
Full Text Sources
