

Artificial Intelligence-Augmented Propensity Score, Cost Effectiveness and Computational Ethical Analysis of Cardiac Arrest and Active Cancer with Novel Mortality Predictive Score
- PMID: 36013506
- PMCID: PMC9412828
- DOI: 10.3390/medicina58081039
Artificial Intelligence-Augmented Propensity Score, Cost Effectiveness and Computational Ethical Analysis of Cardiac Arrest and Active Cancer with Novel Mortality Predictive Score
Abstract
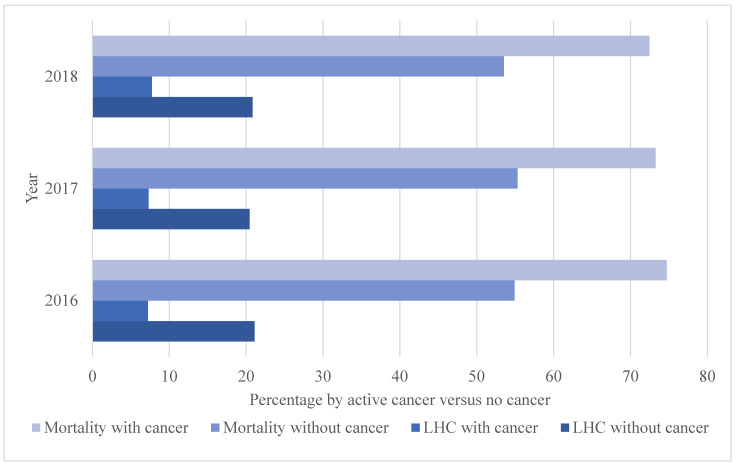
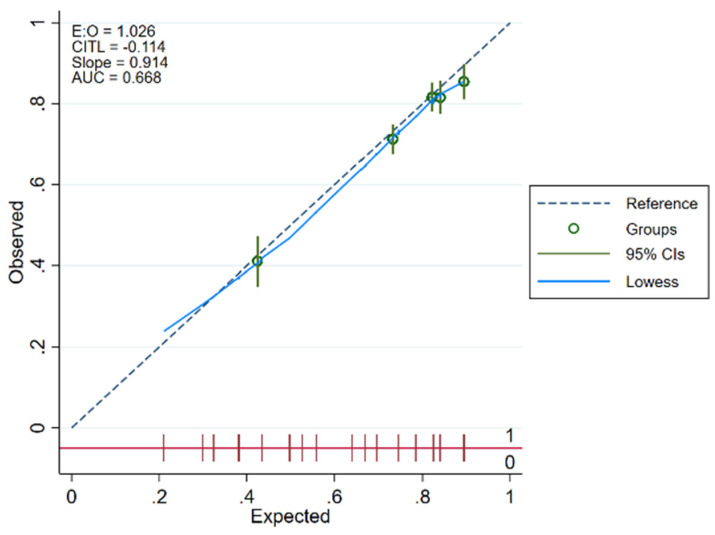
Background and objectives: Little is known about outcome improvements and disparities in cardiac arrest and active cancer. We performed the first known AI and propensity score (PS)-augmented clinical, cost-effectiveness, and computational ethical analysis of cardio-oncology cardiac arrests including left heart catheterization (LHC)-related mortality reduction and related disparities. Materials and methods: A nationally representative cohort analysis was performed for mortality and cost by active cancer using the largest United States all-payer inpatient dataset, the National Inpatient Sample, from 2016 to 2018, using deep learning and machine learning augmented propensity score-adjusted (ML-PS) multivariable regression which informed cost-effectiveness and ethical analyses. The Cardiac Arrest Cardio-Oncology Score (CACOS) was then created for the above population and validated. The results informed the computational ethical analysis to determine ethical and related policy recommendations. Results: Of the 101,521,656 hospitalizations, 6,656,883 (6.56%) suffered cardiac arrest of whom 61,300 (0.92%) had active cancer. Patients with versus without active cancer were significantly less likely to receive an inpatient LHC (7.42% versus 20.79%, p < 0.001). In ML-PS regression in active cancer, post-arrest LHC significantly reduced mortality (OR 0.18, 95%CI 0.14−0.24, p < 0.001) which PS matching confirmed by up to 42.87% (95%CI 35.56−50.18, p < 0.001). The CACOS model included the predictors of no inpatient LHC, PEA initial rhythm, metastatic malignancy, and high-risk malignancy (leukemia, pancreas, liver, biliary, and lung). Cost-benefit analysis indicated 292 racial minorities and $2.16 billion could be saved annually by reducing racial disparities in LHC. Ethical analysis indicated the convergent consensus across diverse belief systems that such disparities should be eliminated to optimize just and equitable outcomes. Conclusions: This AI-guided empirical and ethical analysis provides a novel demonstration of LHC mortality reductions in cardio-oncology cardiac arrest and related disparities, along with an innovative predictive model that can be integrated within the digital ecosystem of modern healthcare systems to improve equitable clinical and public health outcomes.
Keywords: artificial intelligence; cardiac arrest; cardio-oncology; cost effectiveness; equity; ethics.
Conflict of interest statement
None for all authors. DJM provided pro bono analyses.
Figures



Similar articles
-
Percutaneous Coronary Intervention Mortality, Cost, Complications, and Disparities after Radiation Therapy: Artificial Intelligence-Augmented, Cost Effectiveness, and Computational Ethical Analysis.J Cardiovasc Dev Dis. 2023 Oct 30;10(11):445. doi: 10.3390/jcdd10110445. J Cardiovasc Dev Dis. 2023. PMID: 37998503 Free PMC article.
-
Prevalence, mortality, cost, and disparities in transcatheter mitral valve repair and replacement in cancer patients: Artificial intelligence and propensity score national 5-year analysis of 7495 procedures.Int J Cardiol. 2024 Aug 1;408:132091. doi: 10.1016/j.ijcard.2024.132091. Epub 2024 Apr 23. Int J Cardiol. 2024. PMID: 38663811
-
Post-cardiac arrest PCI is underutilized among cancer patients: Machine learning augmented nationally representative case-control study of 30 million hospitalizations.Resuscitation. 2022 Oct;179:43-49. doi: 10.1016/j.resuscitation.2022.07.032. Epub 2022 Aug 4. Resuscitation. 2022. PMID: 35933056
-
Cardio oncology: Digital innovations, precision medicine and health equity.Front Cardiovasc Med. 2022 Nov 3;9:951551. doi: 10.3389/fcvm.2022.951551. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36407451 Free PMC article. Review.
-
Machine Learning in Cardio-Oncology: New Insights from an Emerging Discipline.Rev Cardiovasc Med. 2023 Oct 19;24(10):296. doi: 10.31083/j.rcm2410296. eCollection 2023 Oct. Rev Cardiovasc Med. 2023. PMID: 39077576 Free PMC article. Review.
Cited by
-
Coronary Revascularization in Patients With Cancer.Curr Treat Options Cardiovasc Med. 2023;25(6):143-158. doi: 10.1007/s11936-023-00982-9. Epub 2023 Apr 21. Curr Treat Options Cardiovasc Med. 2023. PMID: 37143711 Free PMC article. Review.
-
Artificial intelligence-augmented analysis of contemporary procedural, mortality, and cost trends in carcinoid heart disease in a large national cohort with a focus on the "forgotten pulmonic valve".Front Cardiovasc Med. 2023 Feb 8;9:1071138. doi: 10.3389/fcvm.2022.1071138. eCollection 2022. Front Cardiovasc Med. 2023. PMID: 36843627 Free PMC article.
-
Can propensity score matching replace randomized controlled trials?World J Methodol. 2024 Mar 20;14(1):90590. doi: 10.5662/wjm.v14.i1.90590. eCollection 2024 Mar 20. World J Methodol. 2024. PMID: 38577204 Free PMC article. Review.
-
Digitalization of health care in low- and middle-income countries.Bull World Health Organ. 2025 Feb 1;103(2):148-154. doi: 10.2471/BLT.24.291643. Epub 2024 Dec 3. Bull World Health Organ. 2025. PMID: 39882493 Free PMC article.
-
Percutaneous Coronary Intervention Mortality, Cost, Complications, and Disparities after Radiation Therapy: Artificial Intelligence-Augmented, Cost Effectiveness, and Computational Ethical Analysis.J Cardiovasc Dev Dis. 2023 Oct 30;10(11):445. doi: 10.3390/jcdd10110445. J Cardiovasc Dev Dis. 2023. PMID: 37998503 Free PMC article.
References
-
- Paratz E.D., Rowsell L., Zentner D., Parsons S., Morgan N., Thompson T., James P., Pflaumer A., Semsarian C., Smith K., et al. Cardiac arrest and sudden cardiac death registries: A systematic review of global coverage. Open Heart. 2020;7:e001195. doi: 10.1136/openhrt-2019-001195. - DOI - PMC - PubMed
-
- Yan S., Gan Y., Jiang N., Wang R., Chen Y., Luo Z., Zong Q., Chen S., Lv C. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: A systematic review and meta-analysis. Crit. Care. 2020;24:61. doi: 10.1186/s13054-020-2773-2. - DOI - PMC - PubMed
-
- Reynolds J.C., Grunau B.E., Rittenberger J.C., Sawyer K.N., Kurz M.C., Callaway C.W. Association between duration of resuscitation and favorable outcome after out-of-hospital cardiac arrest: Implications for prolonging or terminating resuscitation. Circulation. 2016;134:2084–2094. doi: 10.1161/CIRCULATIONAHA.116.023309. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
