

Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE): A Comprehensive Approach and Case Series: Systemic Corticosteroid Therapy Is Necessary in a Large Proportion of Cases
- PMID: 36013537
- PMCID: PMC9415092
- DOI: 10.3390/medicina58081070
Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE): A Comprehensive Approach and Case Series: Systemic Corticosteroid Therapy Is Necessary in a Large Proportion of Cases
Abstract
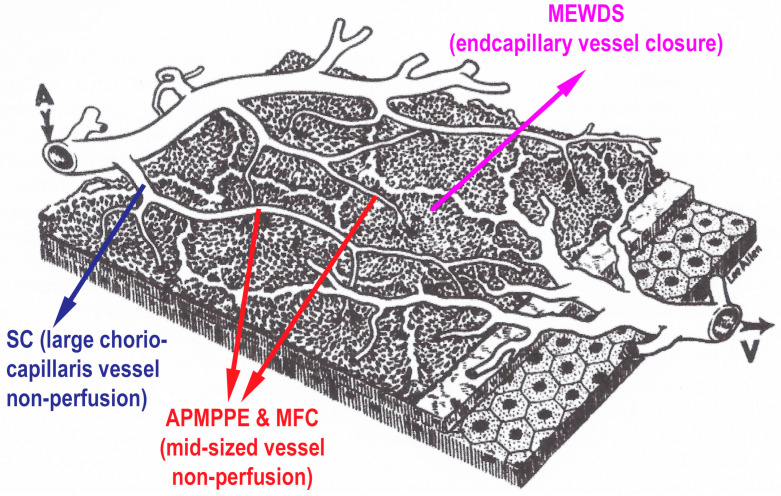
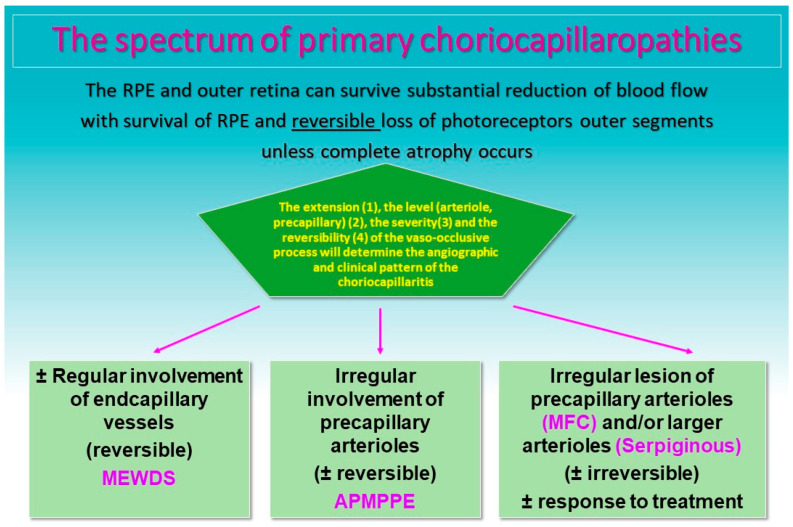
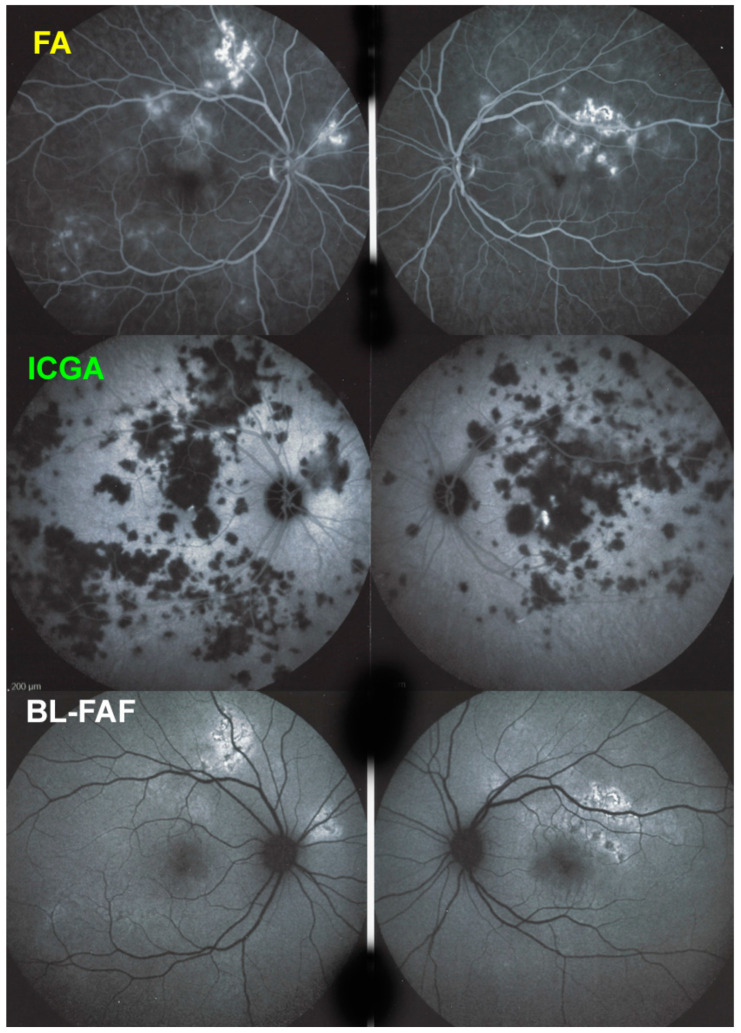
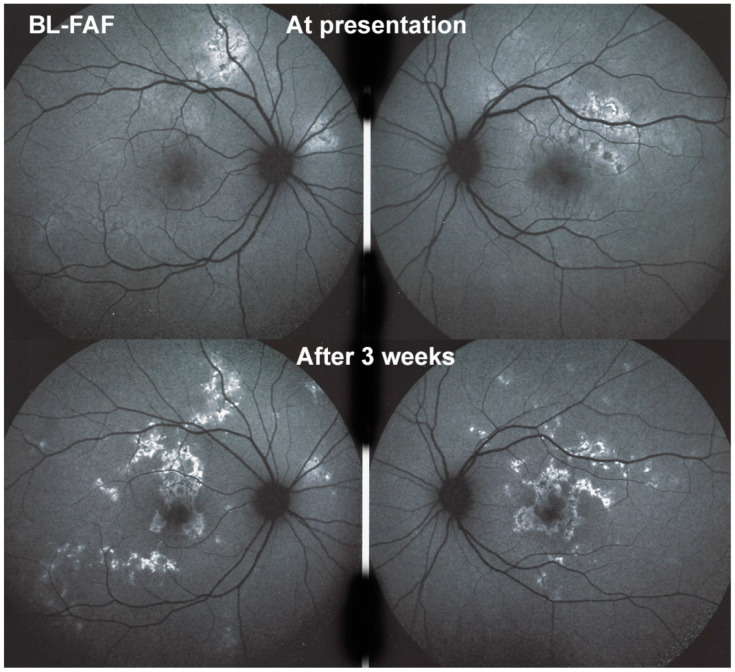
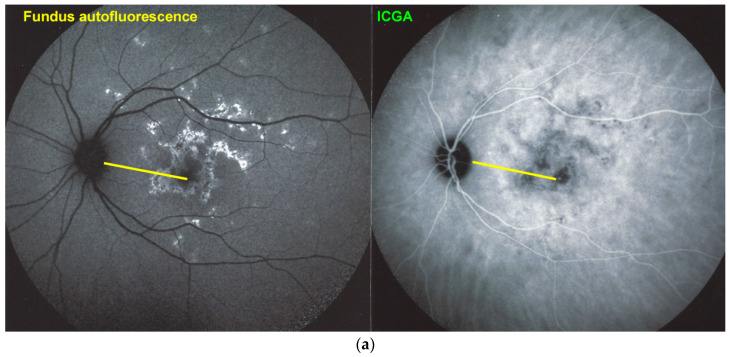
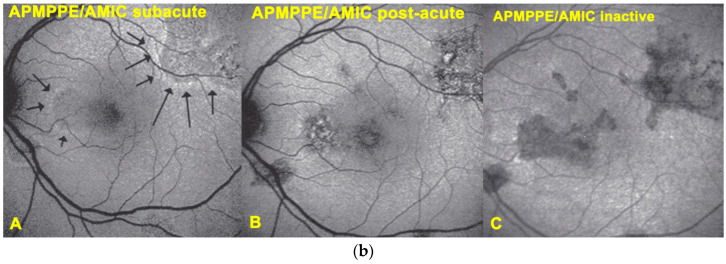
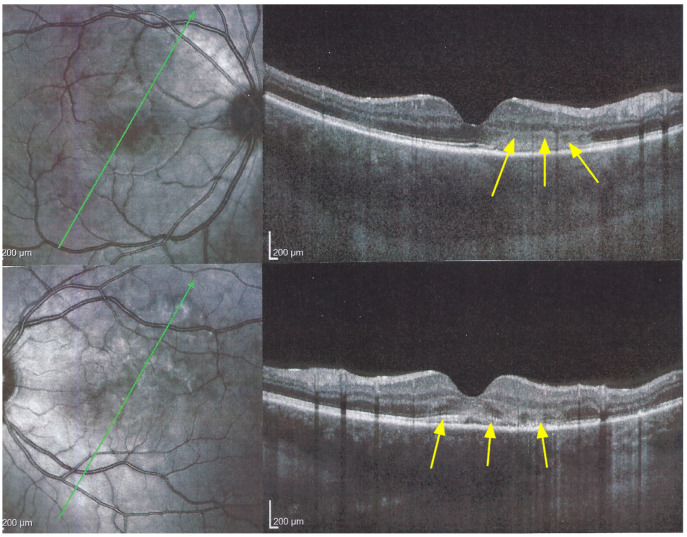
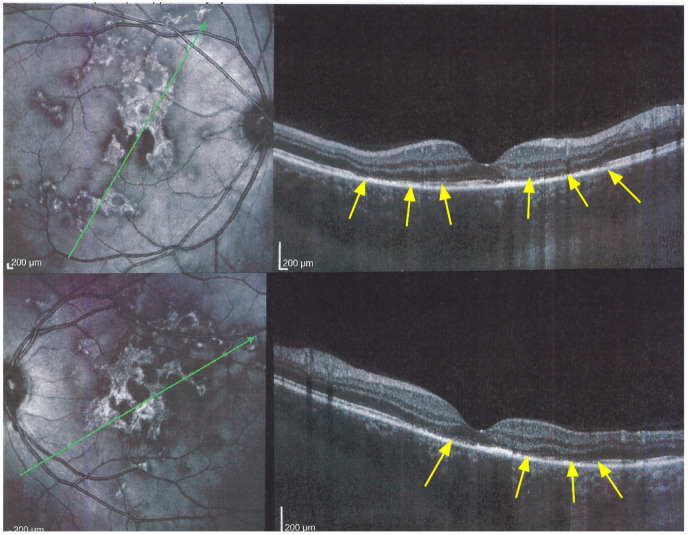
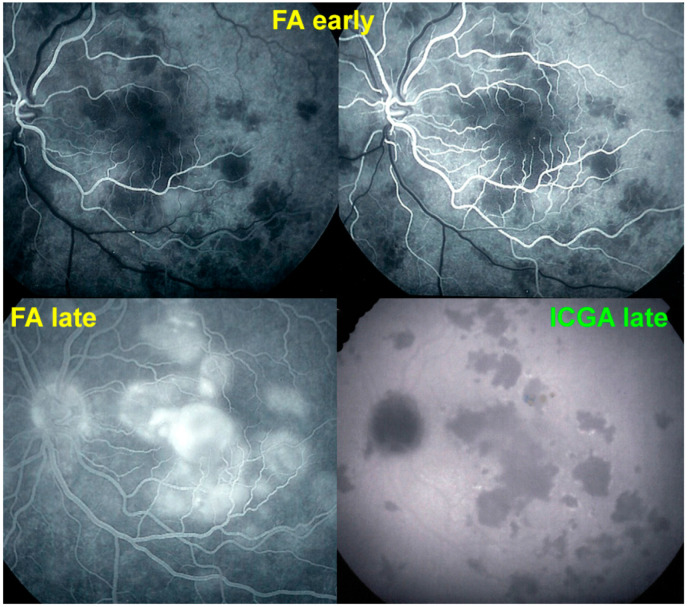
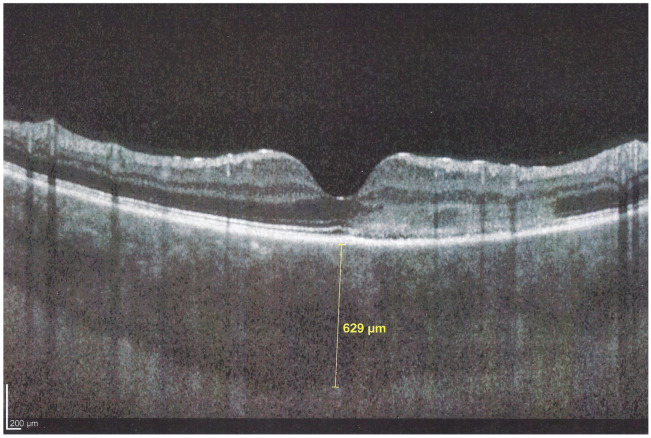
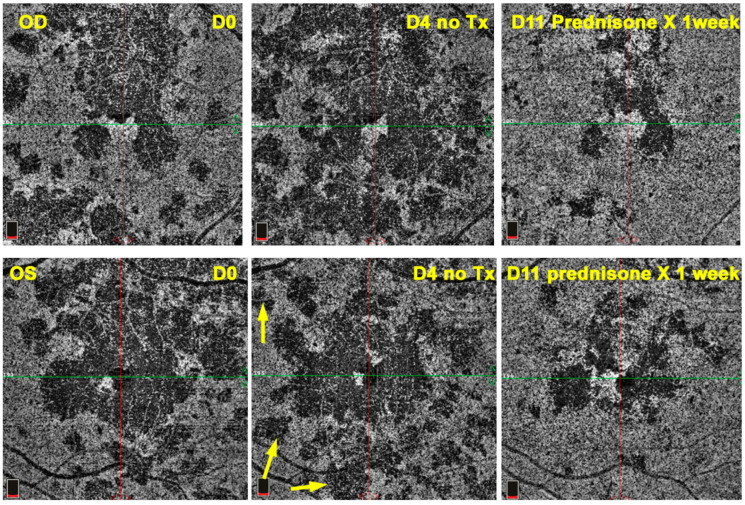
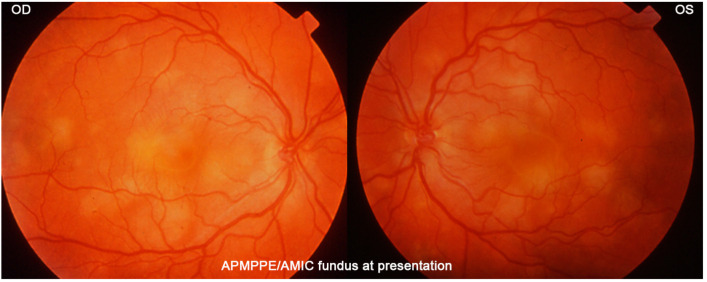
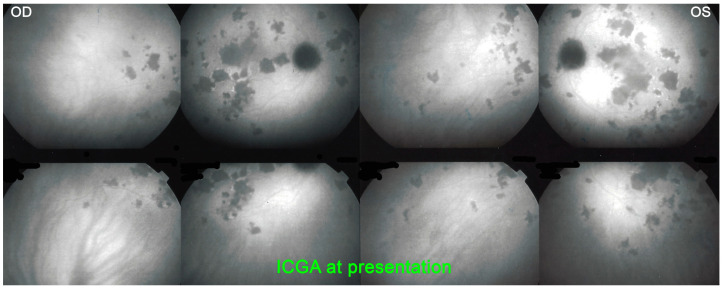
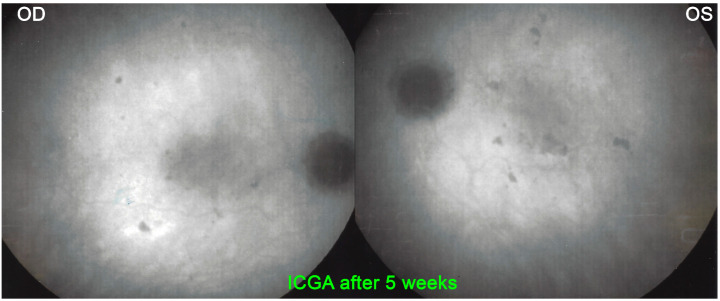
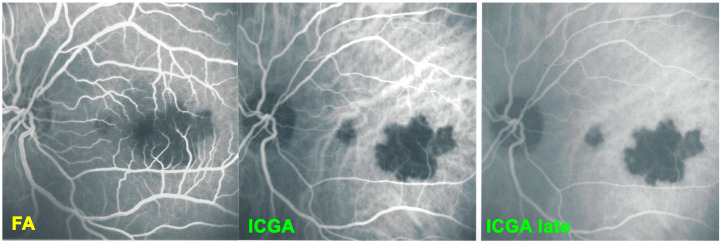
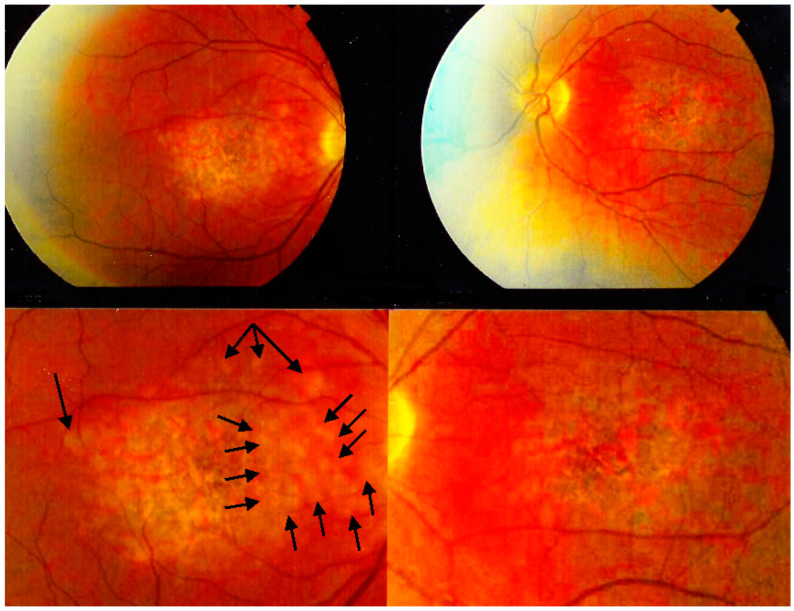
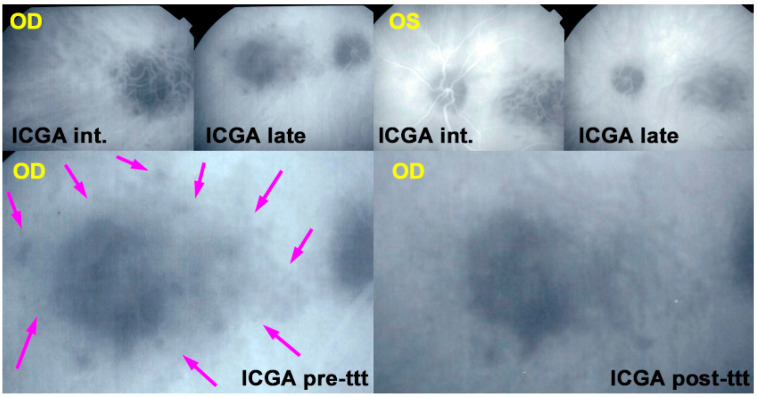
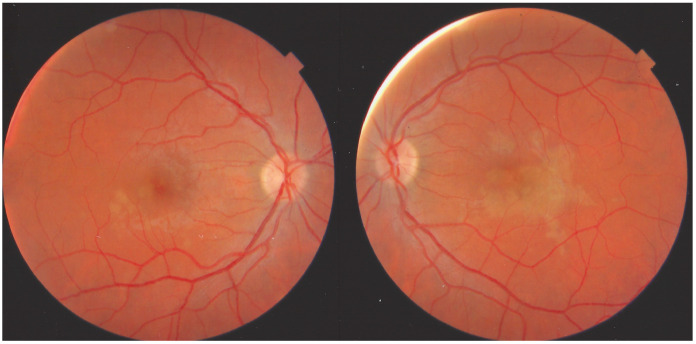
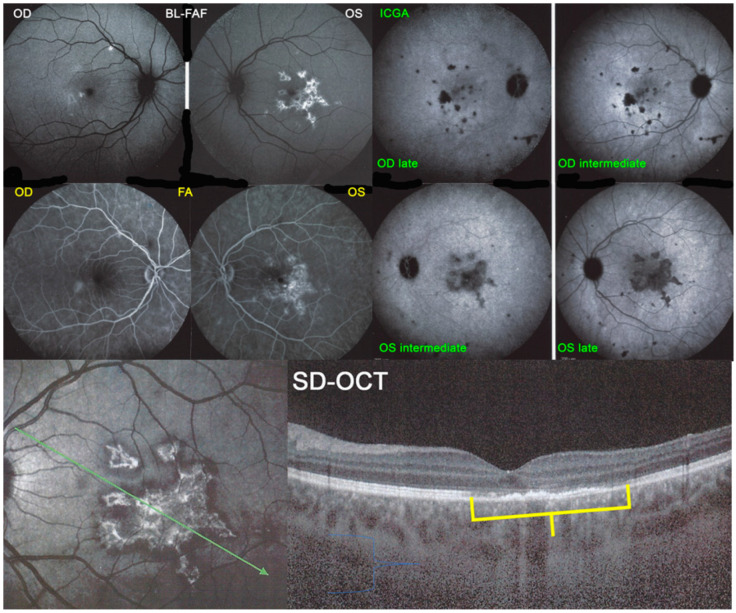
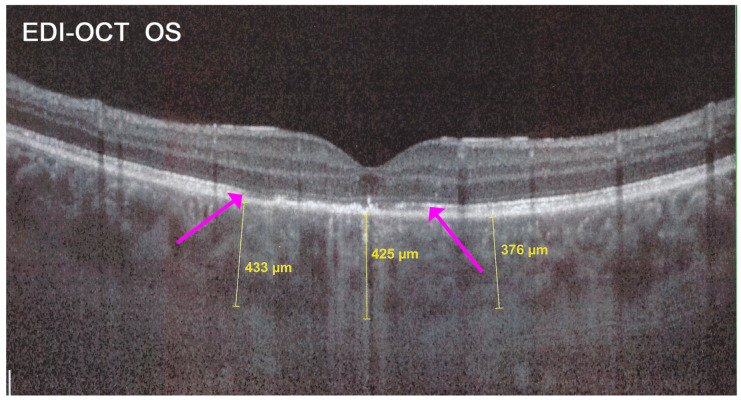
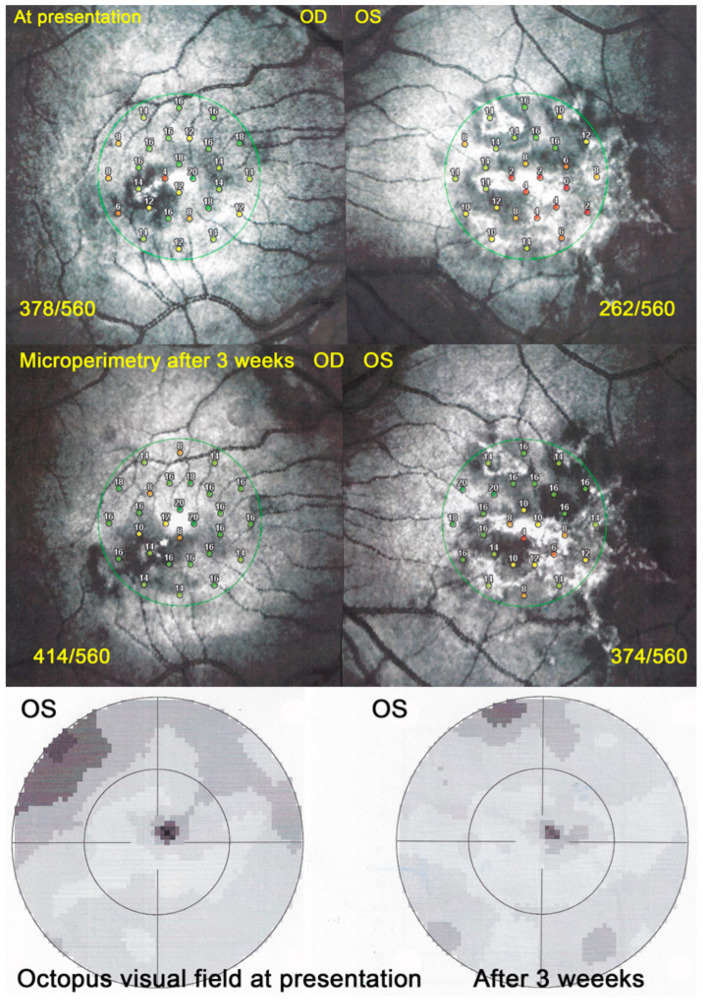
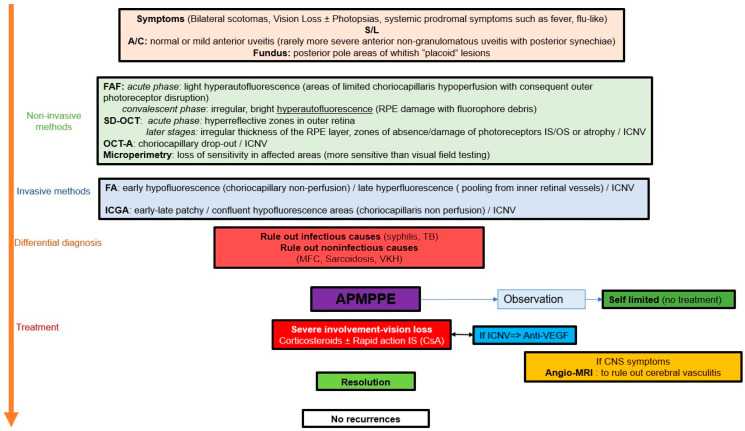
Background and objectives: Acute posterior multifocal pigment epitheliopathy/acute multifocal ischaemic choriocapillaritis (APMPPE/AMIC) is part of the group of choriocapillaritis entities. The aim of this article was to report a series of patients with emphasis on the clinical presentation and treatment paradigms. Materials and Methods: Retrospective case series study performed in the Centre for Ophthalmic Specialised care (COS), Lausanne, Switzerland, on patients diagnosed from 2000 to 2021 with APMPPE/AMIC. Procedures performed at presentation and upon follow-up (when available) included best corrected visual acuity (BCVA), routine ocular examination, laser flare photometry (LFP) microperimetry (when available) and visual field testing. Imaging investigations included spectral domain optical coherence tomography (SD-OCT)/enhanced depth imaging OCT (EDI-OCT), OCT angiography (OCT-A) as well as fluorescein and indocyanine green angiography (FA, ICGA). The presence or not of prodromal systemic viral-like symptoms was noted. The localisation of lesions whether foveal or extrafoveal, divided the patients into 2 groups (foveal, peri-or parafoveal). Exclusion criteria were patients diagnosed with APMPPE/AMIC and a positive QuantiFERON test and/or VDRL-TPHA tests. Results: Nineteen (35 eyes) of 1664 new patients (1.14%) were diagnosed with APMPPE/AMIC and included in our study. 13 (68%) were male and 6 (32%) were female. The mean age was 33.1 ± 9.2 years. 16 (84%) patients mentioned a viral prodromal episode or other systemic symptoms, and 3 (16%) did not mention any episode before the onset of ocular symptoms. 15 (39%) out of 38 eyes had foveal localisation of the lesions, 20 (52.6%) had peri- or para-foveal localisations and 3 eyes were normal [3 unilateral cases (15%)]. Mean BCVA at presentation was 0.83 ± 0.24 for the whole group. It was 0.58 ± 0.28 for the group with foveal lesions, increasing to 0.97 ± 0.13 at last follow-up (p = 0.0028). For the group with extrafoveal lesions mean BCVA at presentation was 0.94 ± 0.18, improving to 1.18± 0.10 at last follow-up (p = 0.0039). 13 (68%) patients received prednisone treatment, of whom 2 (10%) received additionally at least one immunosuppressive agent, 4 (20%) patients received no treatment and in 2 patients the information was unavailable. All patients in the foveal lesion group received corticosteroid treatment except one who evolved to bilateral macular atrophy. Conclusions: APMPPE/AMIC is a primary choriocapillaritis. Although it is thought that the disease is self-limited, treatment is necessary in most cases, especially when lesions are located in the fovea.
Keywords: APMPPE/AMIC; blue light fundus autofluorescence (BL-FAF); enhanced depth imaging OCT (EDI-OCT); indocyanine green angiography (ICGA); primary inflammatory choriocapillaropathies (PICCPs); spectral domain optical coherence tomography (SD-OCT).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
