

Timing and Outcomes of Noninvasive Ventilation in 307 ARDS COVID-19 Patients: An Observational Study in an Italian Third Level COVID-19 Hospital
- PMID: 36013571
- PMCID: PMC9416080
- DOI: 10.3390/medicina58081104
Timing and Outcomes of Noninvasive Ventilation in 307 ARDS COVID-19 Patients: An Observational Study in an Italian Third Level COVID-19 Hospital
Abstract
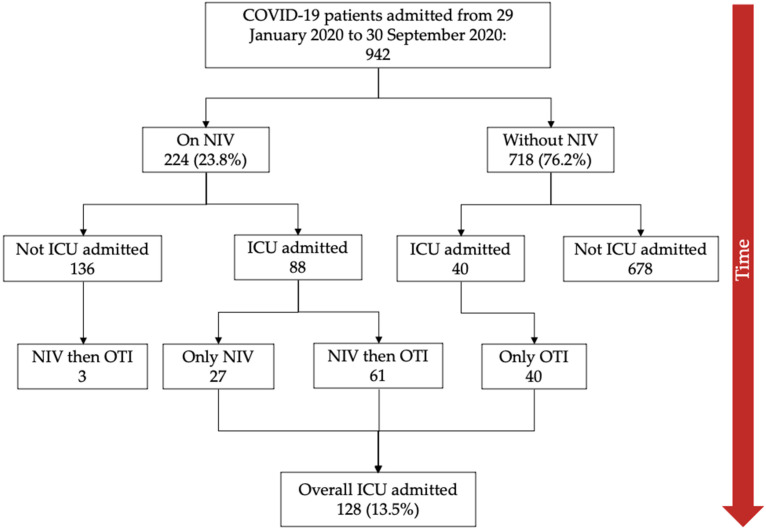
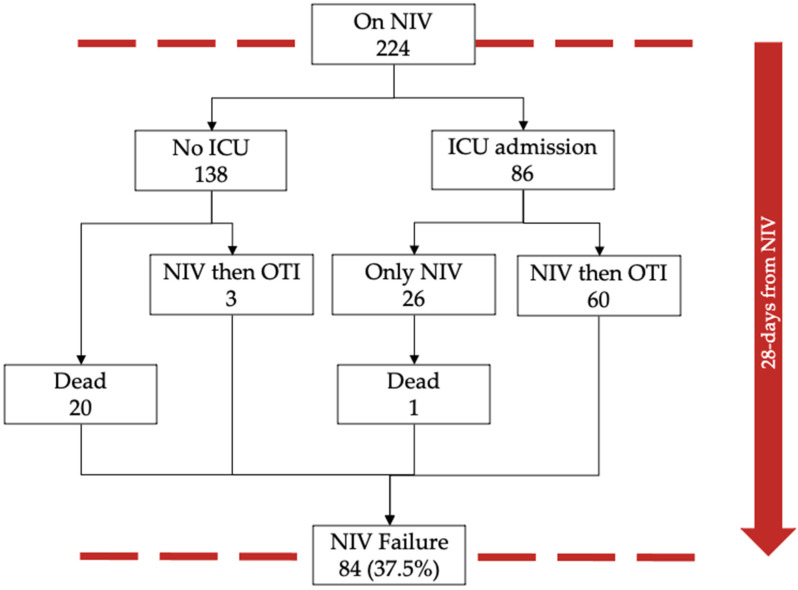
Background and Objectives: Background: Coronavirus disease 2019 (COVID-19) is a novel cause of Acute Respiratory Distress Syndrome (ARDS). Noninvasive ventilation (NIV) is widely used in patients with ARDS across several etiologies. Indeed, with the increase of ARDS cases due to the COVID-19 pandemic, its use has grown significantly in hospital wards. However, there is a lack of evidence to support the efficacy of NIV in patients with COVID-19 ARDS. Materials and Methods: We conducted an observational cohort study including adult ARDS COVID-19 patients admitted in a third level COVID-center in Rome, Italy. The study analyzed the rate of NIV failure defined by the occurrence of orotracheal intubation and/or death within 28 days from starting NIV, its effectiveness, and the associated relative risk of death. The factors associated with the outcomes were identified through logistic regression analysis. Results: During the study period, a total of 942 COVID-19 patients were admitted to our hospital, of which 307 (32.5%) presented with ARDS at hospitalization. During hospitalization 224 (23.8%) were treated with NIV. NIV failure occurred in 84 (37.5%) patients. At 28 days from starting NIV, moderate and severe ARDS had five-fold and twenty-fold independent increased risk of NIV failure (adjusted odds ratio, aOR = 5.01, 95% CI 2.08−12.09, and 19.95, 95% CI 5.31−74.94), respectively, compared to patients with mild ARDS. A total of 128 patients (13.5%) were admitted to the Intensive Care Unit (ICU). At 28-day from ICU admission, intubated COVID-19 patients treated with early NIV had 40% lower mortality (aOR 0.60, 95% CI 0.25−1.46, p = 0.010) compared with patients that underwent orotracheal intubation without prior NIV. Conclusions: These findings show that NIV failure was independently correlated with the severity category of COVID-19 ARDS. The start of NIV in COVID-19 patients with mild ARDS (P/F > 200 mmHg) appears to increase NIV effectiveness and reduce the risk of orotracheal intubation and/or death. Moreover, early NIV (P/F > 200 mmHg) treatment seems to reduce the risk of ICU mortality at 28 days from ICU admission.
Keywords: ARDS; COVID-19; NIV failure; acute respiratory distress syndrome; intensive care unit; noninvasive ventilation; orotracheal intubation.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Figures

References
-
- WHO Coronavirus Disease (COVID-19) Dashboard|WHO Coronavirus Disease (COVID-19) Dashboard. [(accessed on 27 May 2022)]. Available online: https://covid19.who.int/
-
- CDC Infection Control: Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2)|CDC. [(accessed on 27 May 2022)]; Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control.html.
-
- Ferguson N.D., Fan E., Camporota L., Antonelli M., Anzueto A., Beale R., Brochard L., Brower R., Esteban A., Gattinoni L., et al. The Berlin Definition of ARDS: An Expanded Rationale, Justification, and Supplementary Material. Intensive Care Med. 2012;38:1573–1582. doi: 10.1007/s00134-012-2682-1. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
