

Consortium of Indigenous Fecal Bacteria in the Treatment of Metabolic Syndrome
- PMID: 36013992
- PMCID: PMC9414820
- DOI: 10.3390/microorganisms10081574
Consortium of Indigenous Fecal Bacteria in the Treatment of Metabolic Syndrome
Abstract
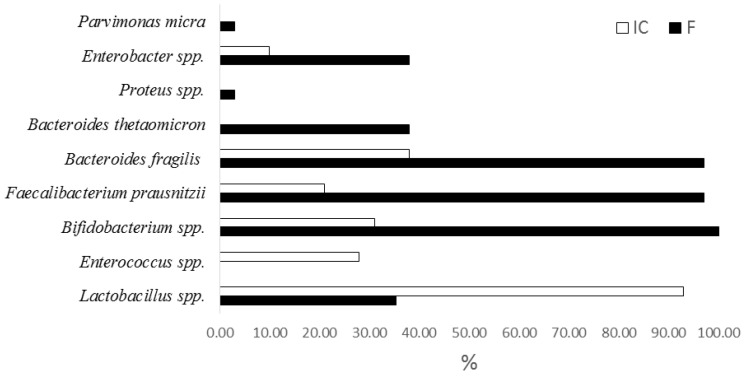
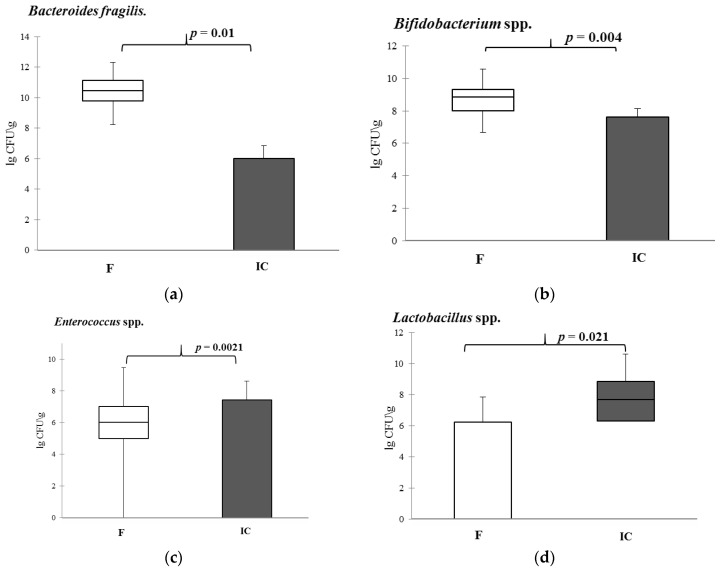
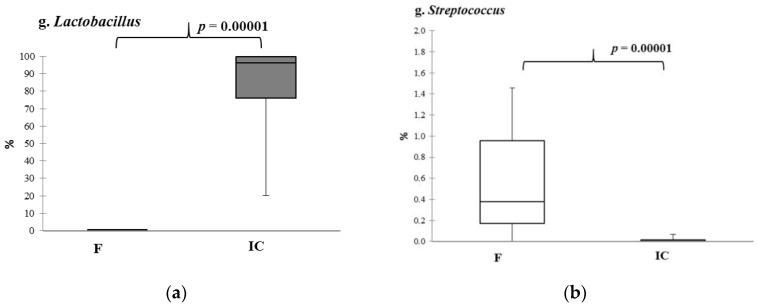
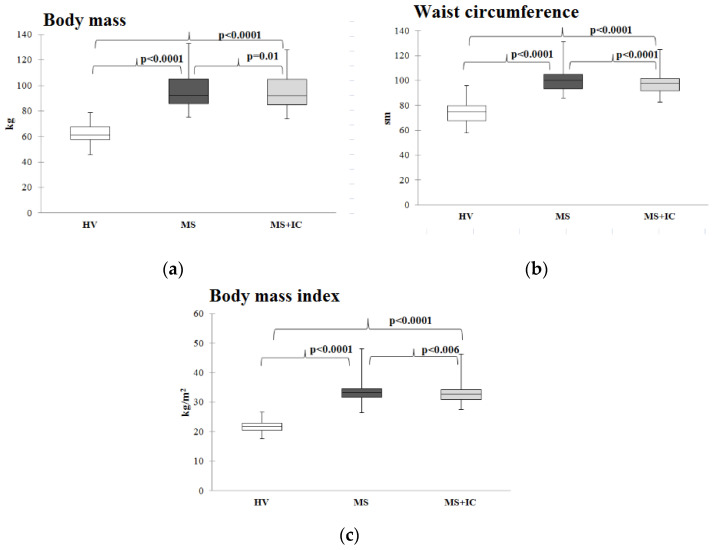
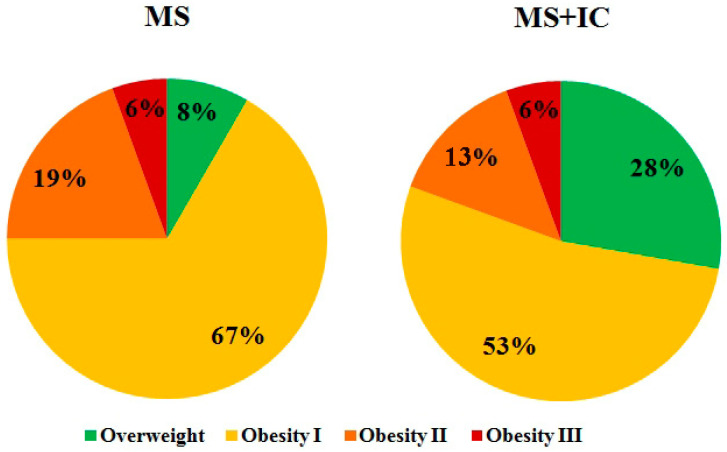
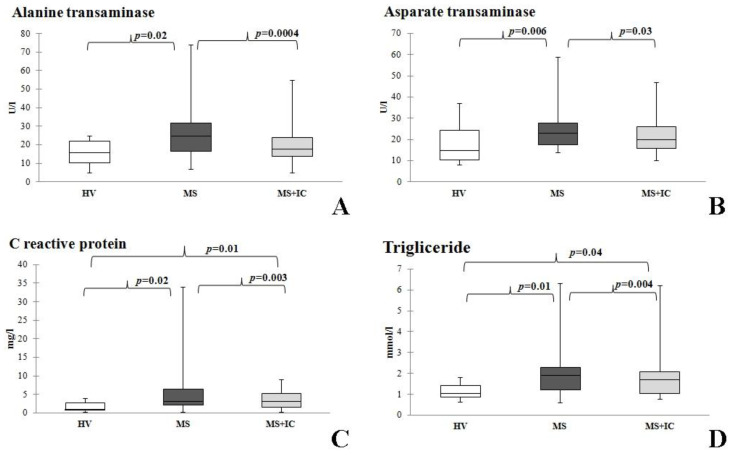
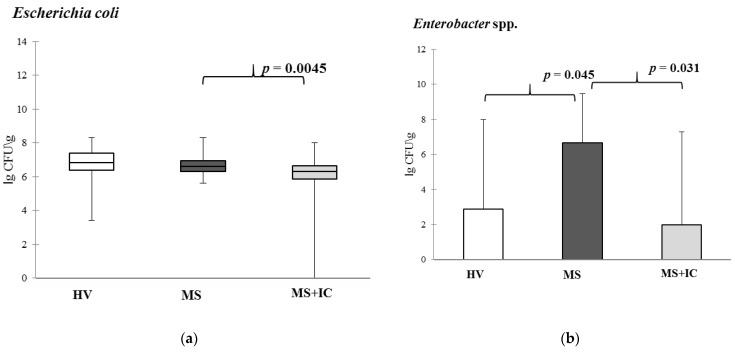
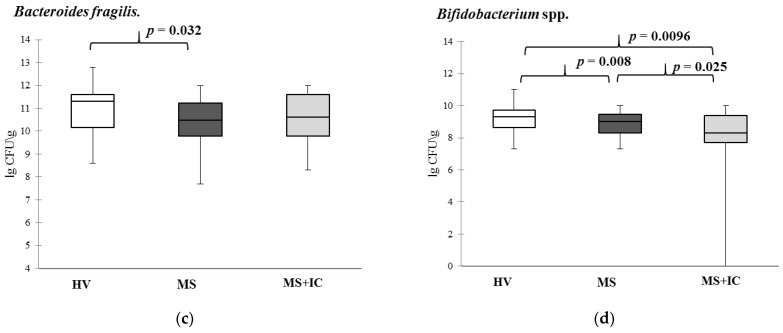
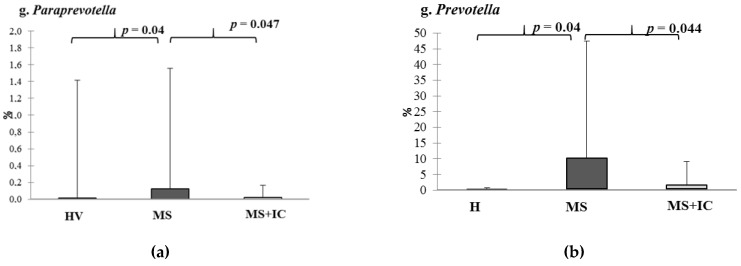
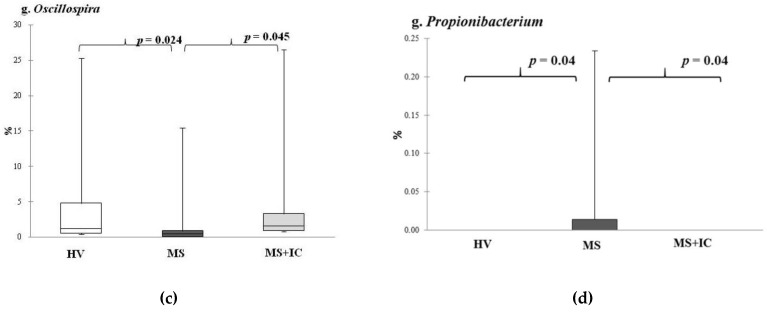
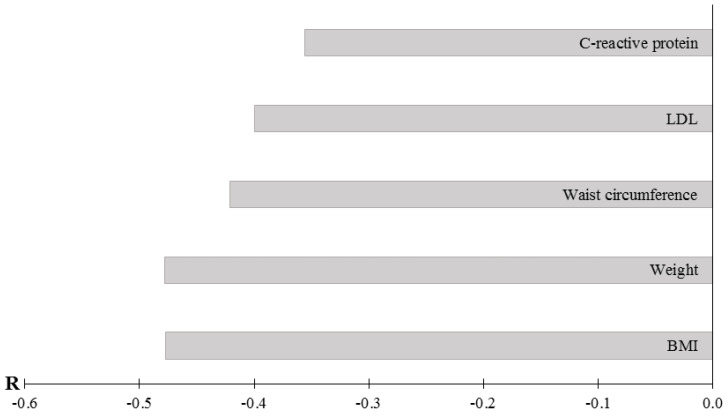
The features of gut microbiota in metabolic syndrome (MS) and ways to correct it using autoprobiotics, based on indigenous bacteria obtained from fecal samples of the host, remain unexplored. The aim of the study was to investigate the effectiveness of an indigenous consortium (IC) of fecal bacteria in treatment of patients with MS. The study was carried out on 36 patients with MS, manifested with abdominal obesity, eating disorders, dyslipidemia, and hypertension. The control group was formed by 20 healthy volunteers. Samples of IC and gut microbiota content were examined by qPCR and metagenome (16S rRNA) analysis before and after therapy. The decrease in anthropometric parameters of obesity, liver enzyme level correction, reduction in C reactive protein and triglyceride concentrations were revealed after IC usage. The decrease in genera Bifidobacterium, Enterobacter, Paraprevotella, and Prevotella, as well as an increase in Bacteroides fragilis and Oscillospira spp. populations were shown after consumption of IC. A negative correlation between the quantity of B. fragilis and the anthropometric parameters of obesity (r = -0.48) and C reactive protein level (r = -0.36) in serum was established. Thus, IC can be considered as a potential functional personified product for the therapy of MS.
Keywords: Bacteroides fragilis; Bifidobacterium spp.; Lactobacillus spp.; autoprobiotics; dyslipidemia; eating disorders; indigenous consortium; obesity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kurmangulov A.A., Dorodneva E.F., Isakova D.N. Functional activity of intestinal microbiota with metabolic syndrome. Obes. Metab. 2016;13:16–19. doi: 10.14341/omet2016116-19. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
