

Heart Failure with Preserved Ejection Fraction and Pulmonary Hypertension: Focus on Phosphodiesterase Inhibitors
- PMID: 36015172
- PMCID: PMC9414416
- DOI: 10.3390/ph15081024
Heart Failure with Preserved Ejection Fraction and Pulmonary Hypertension: Focus on Phosphodiesterase Inhibitors
Abstract
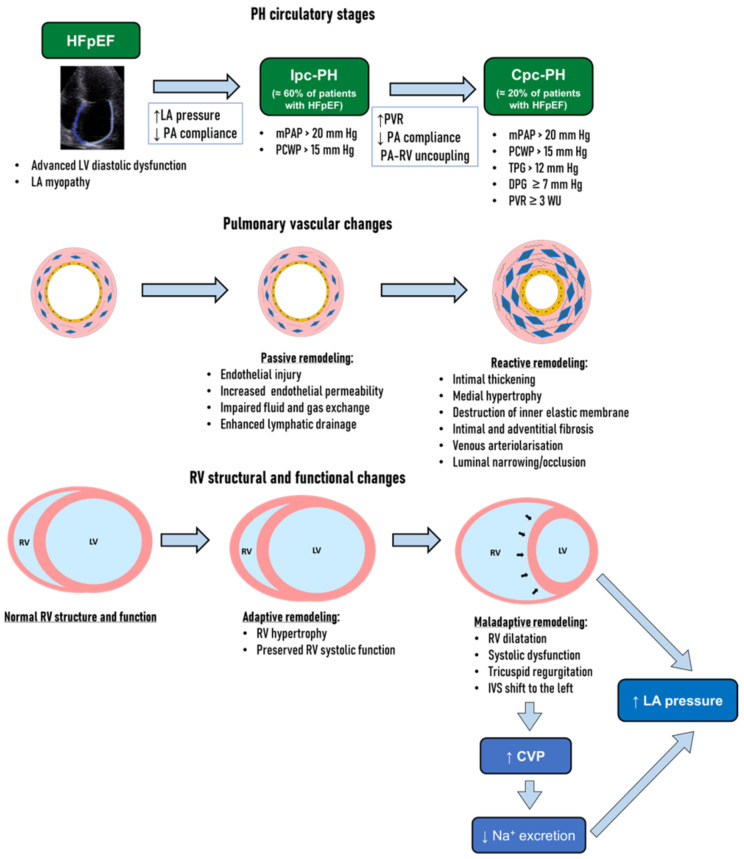
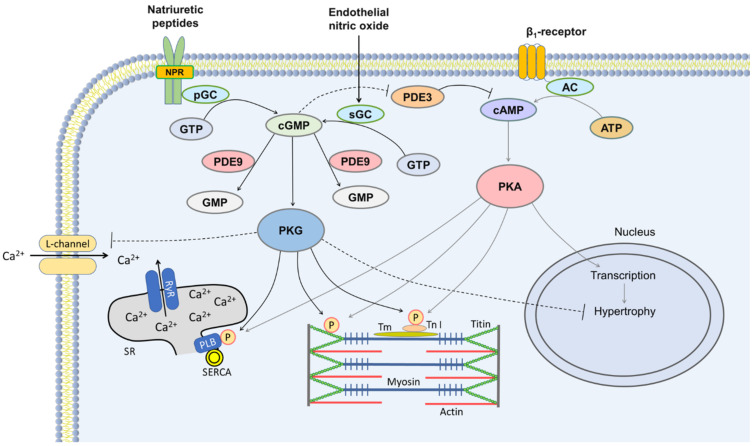
Pulmonary hypertension (PH) is common in patients with heart failure with preserved ejection fraction (HFpEF). A chronic increase in mean left atrial pressure leads to passive remodeling in pulmonary veins and capillaries and modest PH (isolated postcapillary PH, Ipc-PH) and is not associated with significant right ventricular dysfunction. In approximately 20% of patients with HFpEF, "precapillary" alterations of pulmonary vasculature occur with the development of the combined pre- and post-capillary PH (Cpc-PH), pertaining to a poor prognosis. Current data indicate that pulmonary vasculopathy may be at least partially reversible and thus serves as a therapeutic target in HFpEF. Pulmonary vascular targeted therapies, including phosphodiesterase (PDE) inhibitors, may have a valuable role in the management of patients with PH-HFpEF. In studies of Cpc-PH and HFpEF, PDE type 5 inhibitors were effective in long-term follow-up, decreasing pulmonary artery pressure and improving RV contractility, whereas studies of Ipc-PH did not show any benefit. Randomized trials are essential to elucidate the actual value of PDE inhibition in selected patients with PH-HFpEF, especially in those with invasively confirmed Cpc-PH who are most likely to benefit from such treatment.
Keywords: PDE inhibitors; diastolic dysfunction; heart failure with preserved ejection fraction; phosphodiesterase; pulmonary hypertension.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Phosphodiesterase inhibitor for heart failure with preserved ejection fraction: A systematic review and meta-analysis.Saudi Pharm J. 2022 Aug;30(8):1079-1087. doi: 10.1016/j.jsps.2022.05.012. Epub 2022 Jun 1. Saudi Pharm J. 2022. PMID: 36164567 Free PMC article.
-
Phosphodiesterase 5 inhibitor sildenafil in patients with heart failure with preserved ejection fraction and combined pre- and postcapillary pulmonary hypertension: a randomized open-label pilot study.BMC Cardiovasc Disord. 2020 Sep 10;20(1):408. doi: 10.1186/s12872-020-01671-2. BMC Cardiovasc Disord. 2020. PMID: 32912157 Free PMC article. Clinical Trial.
-
Therapeutic potential of phosphodiesterase type 5 inhibitors in heart failure with preserved ejection fraction and combined post- and pre-capillary pulmonary hypertension.Int J Cardiol. 2019 May 15;283:152-158. doi: 10.1016/j.ijcard.2018.12.078. Epub 2019 Jan 4. Int J Cardiol. 2019. PMID: 30777406
-
Management of Pulmonary Hypertension in the Context of Heart Failure with Preserved Ejection Fraction.Curr Hypertens Rep. 2024 Jul;26(7):291-306. doi: 10.1007/s11906-024-01296-2. Epub 2024 Apr 1. Curr Hypertens Rep. 2024. PMID: 38558124 Review.
-
Insights into the pulmonary vascular complications of heart failure with preserved ejection fraction.J Physiol. 2019 Feb;597(4):1143-1156. doi: 10.1113/JP275858. Epub 2018 Dec 30. J Physiol. 2019. PMID: 30549058 Free PMC article. Review.
Cited by
-
Novel insights into the pathobiology of pulmonary hypertension in heart failure with preserved ejection fraction.Am J Physiol Heart Circ Physiol. 2024 Jun 1;326(6):H1498-H1514. doi: 10.1152/ajpheart.00068.2024. Epub 2024 Apr 19. Am J Physiol Heart Circ Physiol. 2024. PMID: 38639739 Free PMC article. Review.
-
Pulmonary vasodilators in patients with advanced chronic kidney disease and pre-capillary pulmonary hypertension-A case series.Respirol Case Rep. 2024 Sep 19;12(9):e70027. doi: 10.1002/rcr2.70027. eCollection 2024 Sep. Respirol Case Rep. 2024. PMID: 39301149 Free PMC article.
-
Pulmonary Hypertension: Pharmacological and Non-Pharmacological Therapies.Life (Basel). 2024 Oct 4;14(10):1265. doi: 10.3390/life14101265. Life (Basel). 2024. PMID: 39459565 Free PMC article. Review.
References
-
- Vasan R.S., Xanthakis V., Lyass A., Andersson C., Tsao C., Cheng S., Aragam J., Benjamin E.J., Larson M.G. Epidemiology of Left Ventricular Systolic Dysfunction and Heart Failure in the Framingham Study: An Echocardiographic Study over 3 Decades. JACC Cardiovasc. Imaging. 2018;11:1–11. doi: 10.1016/j.jcmg.2017.08.007. - DOI - PMC - PubMed
-
- Anker S.D., Butler J., Filippatos G., Ferreira J.P., Bocchi E., Böhm M., Brunner-La Rocca H.P., Choi D.J., Chopra V., Chuquiure-Valenzuela E., et al. EMPEROR-Preserved Trial Investigators. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021;385:1451–1461. doi: 10.1056/NEJMoa2107038. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
