

Progress in 3D Bioprinting Technology for Osteochondral Regeneration
- PMID: 36015207
- PMCID: PMC9414312
- DOI: 10.3390/pharmaceutics14081578
Progress in 3D Bioprinting Technology for Osteochondral Regeneration
Abstract
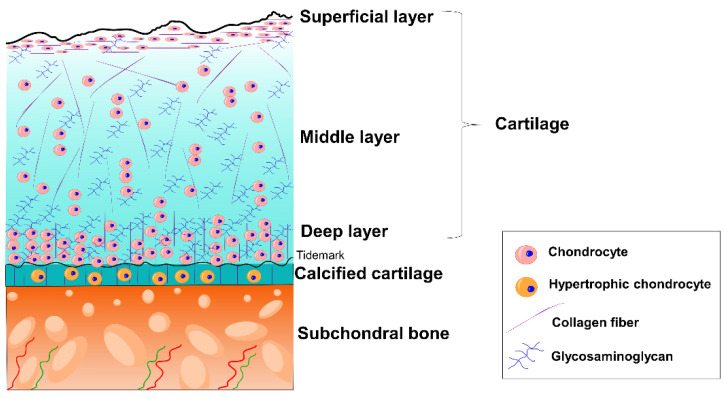
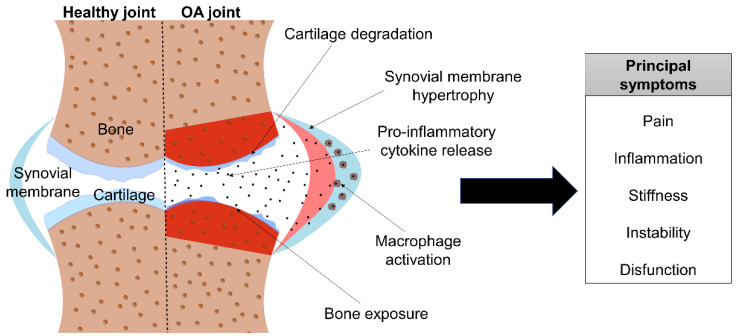
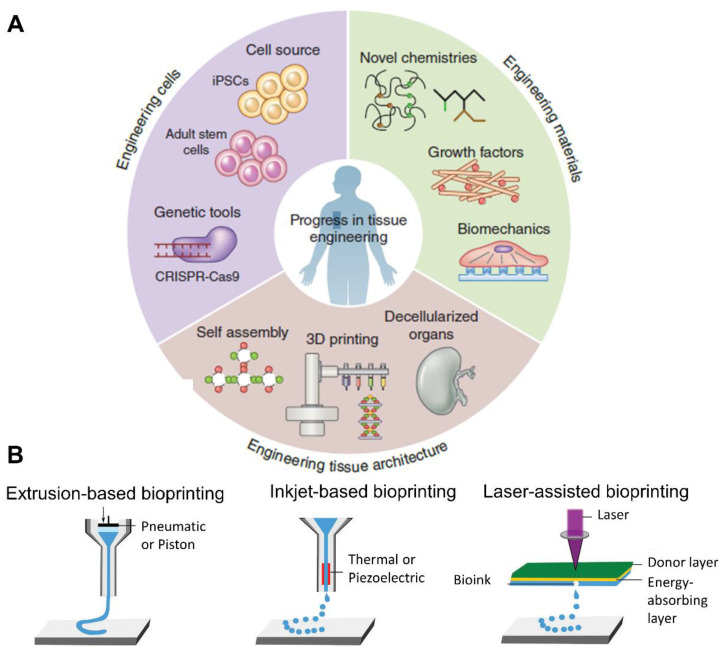
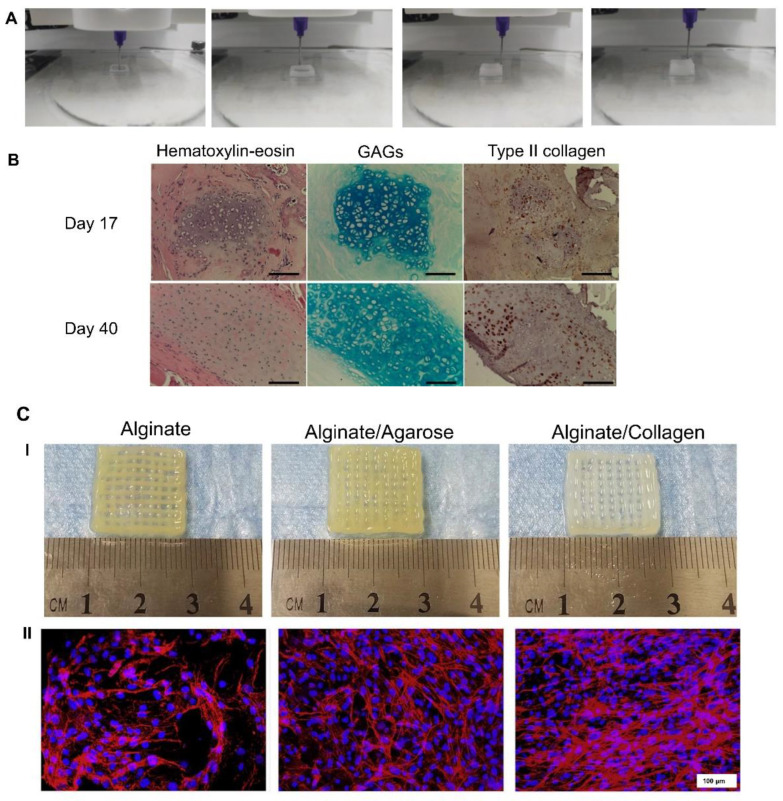
Osteochondral injuries can lead to osteoarthritis (OA). OA is characterized by the progressive degradation of the cartilage tissue together with bone tissue turnover. Consequently, joint pain, inflammation, and stiffness are common, with joint immobility and dysfunction being the most severe symptoms. The increase in the age of the population, along with the increase in risk factors such as obesity, has led OA to the forefront of disabling diseases. In addition, it not only has an increasing prevalence, but is also an economic burden for health systems. Current treatments are focused on relieving pain and inflammation, but they become ineffective as the disease progresses. Therefore, new therapeutic approaches, such as tissue engineering and 3D bioprinting, have emerged. In this review, the advantages of using 3D bioprinting techniques for osteochondral regeneration are described. Furthermore, the biomaterials, cell types, and active molecules that are commonly used for these purposes are indicated. Finally, the most recent promising results for the regeneration of cartilage, bone, and/or the osteochondral unit through 3D bioprinting technologies are considered, as this could be a feasible therapeutic approach to the treatment of OA.
Keywords: 3D bioprinting; bone; cartilage; osteoarthritis; regenerative medicine; tissue engineering.
Conflict of interest statement
The authors declare no conflict of interest. The company had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
Figures





References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
