

Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis
- PMID: 36016242
- PMCID: PMC9412456
- DOI: 10.3390/vaccines10081356
Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis
Abstract
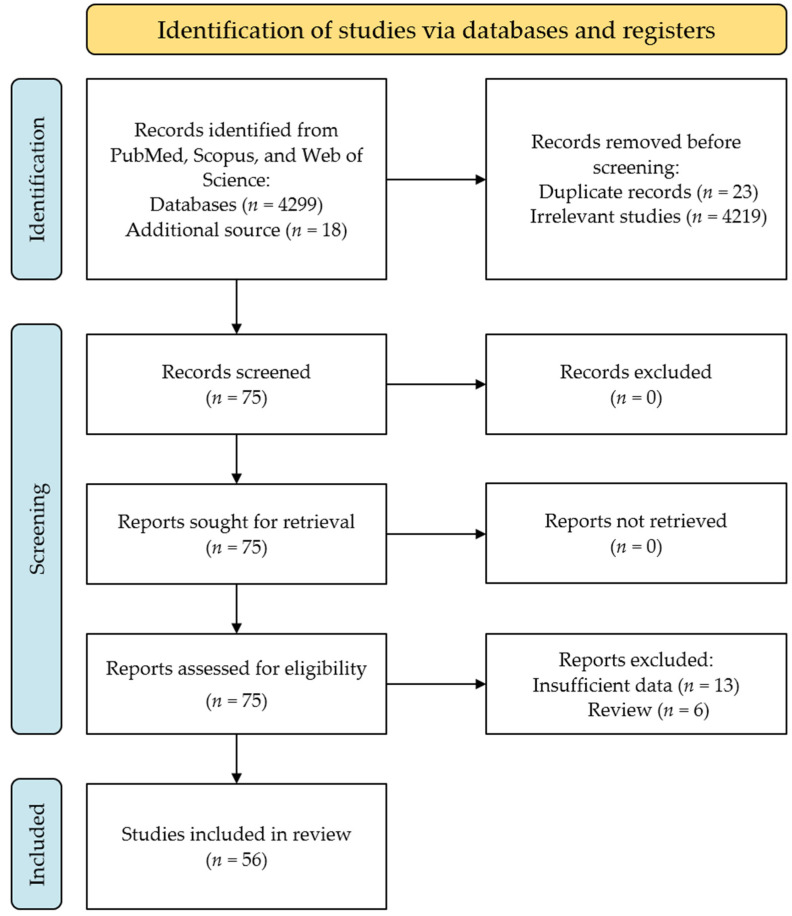
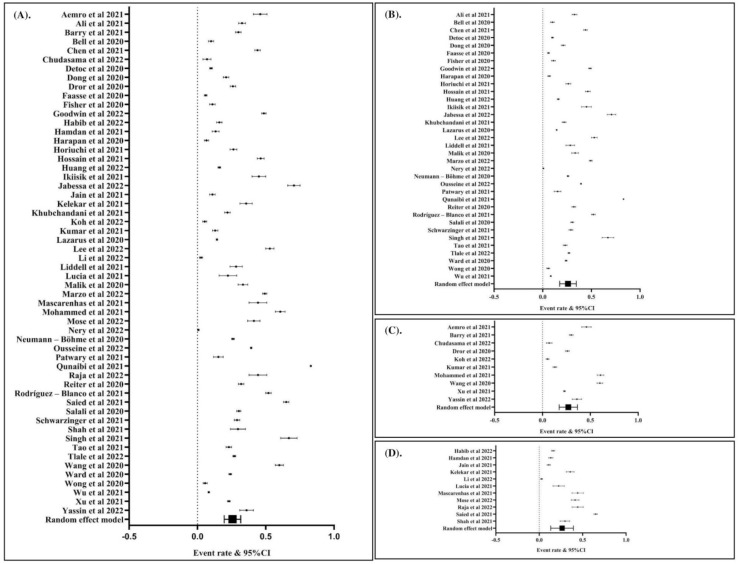
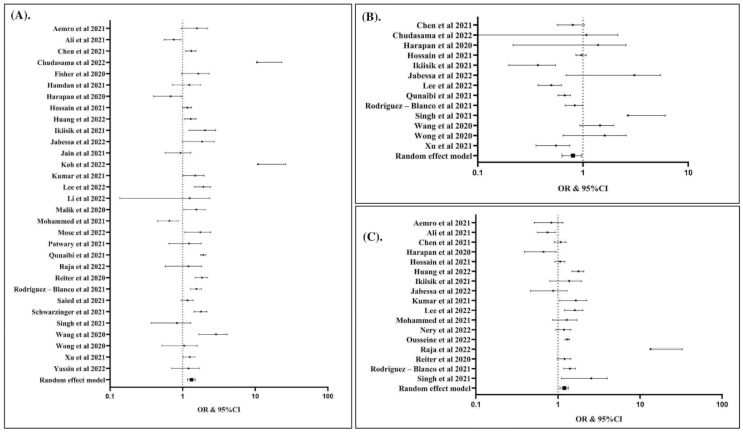
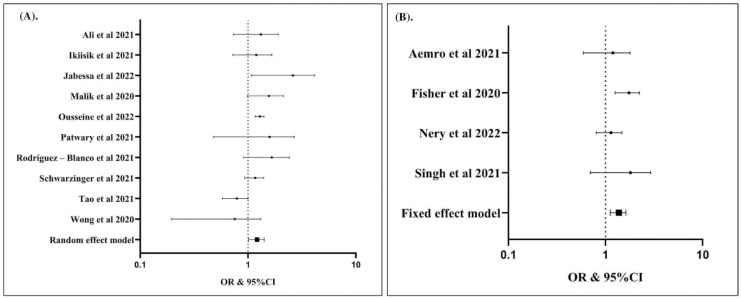
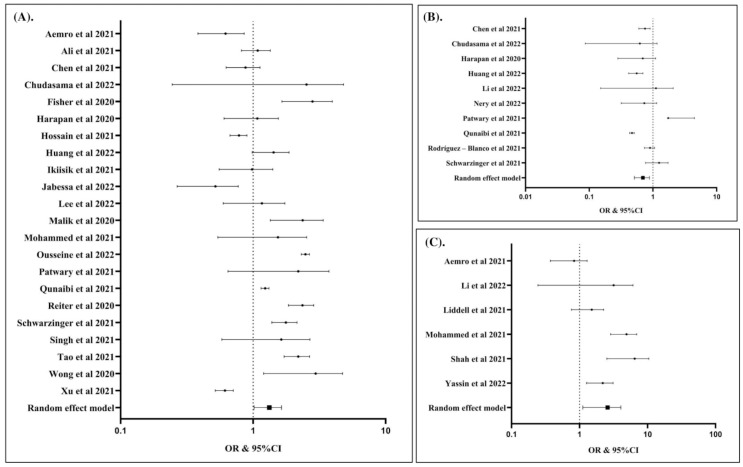
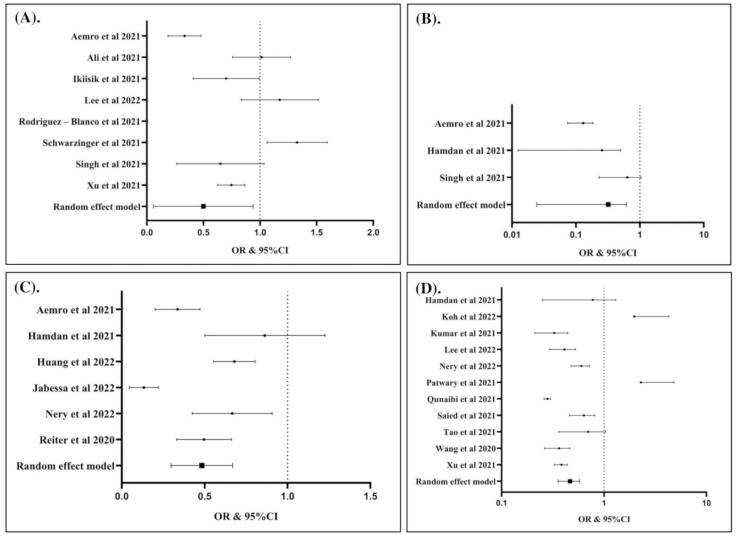
Countries worldwide have deployed mass COVID-19 vaccination drives, but there are people who are hesitant to receive the vaccine. Studies assessing the factors associated with COVID-19 vaccination hesitancy are inconclusive. This study aimed to assess the global prevalence of COVID-19 vaccination hesitancy and determine the potential factors associated with such hesitancy. We performed an organized search for relevant articles in PubMed, Scopus, and Web of Science. Extraction of the required information was performed for each study. A single-arm meta-analysis was performed to determine the global prevalence of COVID-19 vaccination hesitancy; the potential factors related to vaccine hesitancy were analyzed using a Z-test. A total of 56 articles were included in our analysis. We found that the global prevalence of COVID-19 vaccination hesitancy was 25%. Being a woman, being a 50-year-old or younger, being single, being unemployed, living in a household with five or more individuals, having an educational attainment lower than an undergraduate degree, having a non-healthcare-related job and considering COVID-19 vaccines to be unsafe were associated with a higher risk of vaccination hesitancy. In contrast, living with children at home, maintaining physical distancing norms, having ever tested for COVID-19, and having a history of influenza vaccination in the past few years were associated with a lower risk of hesitancy to COVID-19 vaccination. Our study provides valuable information on COVID-19 vaccination hesitancy, and we recommend special interventions in the sub-populations with increased risk to reduce COVID-19 vaccine hesitancy.
Keywords: COVID-19; acceptance; hesitancy; prevalence; vaccination.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Salo H., Kilpi T. National vaccination program—A success story of public health and economy. Duodecim. 2017;133:977–983. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
