

Cancer therapy's impact on lipid metabolism: Mechanisms and future avenues
- PMID: 36017084
- PMCID: PMC9396263
- DOI: 10.3389/fcvm.2022.925816
Cancer therapy's impact on lipid metabolism: Mechanisms and future avenues
Abstract
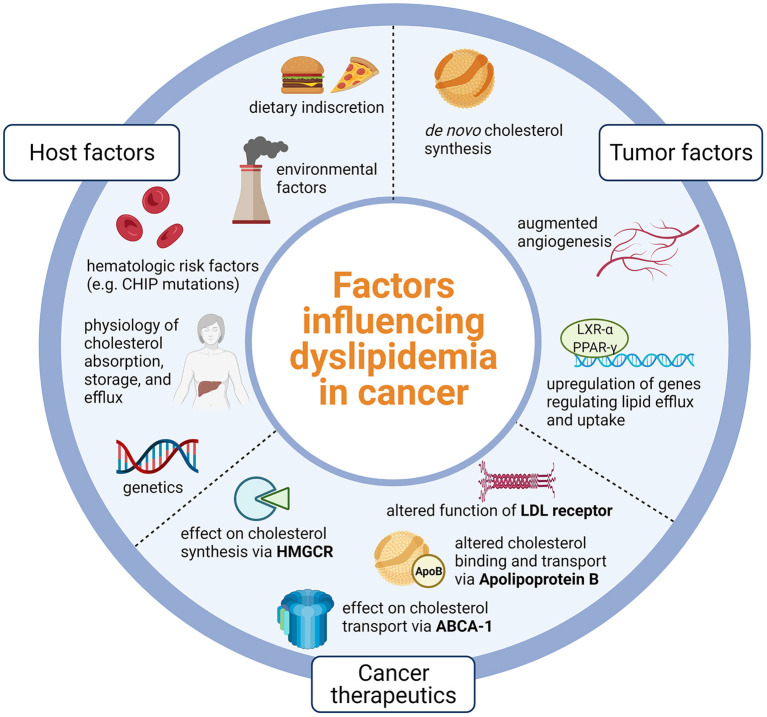
Atherosclerotic cardiovascular disease is a growing threat among cancer patients. Not surprisingly, cancer-targeting therapies have been linked to metabolic dysregulation including changes in local and systemic lipid metabolism. Thus, tumor development and cancer therapeutics are intimately linked to cholesterol metabolism and may be a driver of increased cardiovascular morbidity and mortality in this population. Chemotherapeutic agents affect lipid metabolism through diverse mechanisms. In this review, we highlight the mechanistic and clinical evidence linking commonly used cytotoxic therapies with cholesterol metabolism and potential opportunities to limit atherosclerotic risk in this patient population. Better understanding of the link between atherosclerosis, cancer therapy, and cholesterol metabolism may inform optimal lipid therapy for cancer patients and mitigate cardiovascular disease burden.
Keywords: atherosclerotic disease; chemotherapy; cytotoxic therapy; lipid metabolism; metabolic dysregulation; tumor microenvironment.
Copyright © 2022 Bhatnagar, Dixit, Yang and Sallam.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Ference BA, Ginsberg HN, Graham I, Ray KK, Packard CJ, Bruckert E, et al. . Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the european atherosclerosis society consensus panel. Euro Heart J. (2017) 38:2459–72. 10.1093/eurheartj/ehx144 - DOI - PMC - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. . 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. (2019) 73:3168–209. 10.1016/j.jacc.2018.11.004 - DOI - PubMed