

First-in-human pilot trial of combined intracoronary and intravenous mesenchymal stem cell therapy in acute myocardial infarction
- PMID: 36017096
- PMCID: PMC9395611
- DOI: 10.3389/fcvm.2022.961920
First-in-human pilot trial of combined intracoronary and intravenous mesenchymal stem cell therapy in acute myocardial infarction
Abstract
Background: Acute ST-elevation myocardial infarction (STEMI) elicits a robust cardiomyocyte death and inflammatory responses despite timely revascularization.
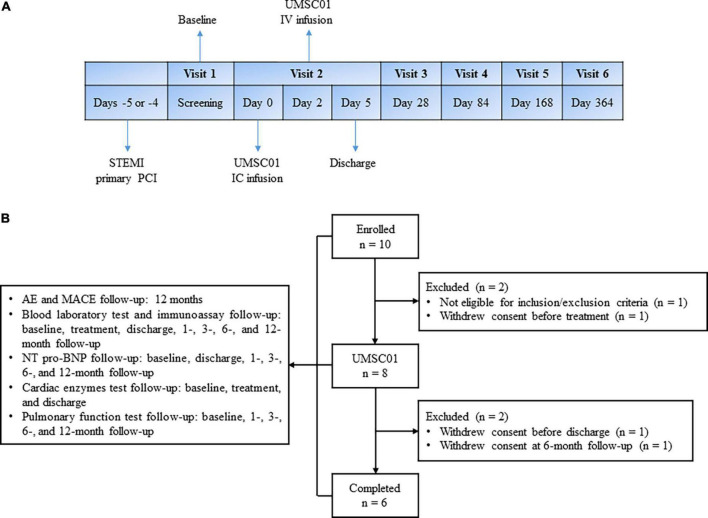
Objectives: This phase 1, open-label, single-arm, first-in-human study aimed to assess the safety and efficacy of combined intracoronary (IC) and intravenous (IV) transplantation of umbilical cord-derived mesenchymal stem cells (UMSC01) for heart repair in STEMI patients with impaired left ventricular ejection fraction (LVEF 30-49%) following successful reperfusion by percutaneous coronary intervention.
Methods: Consenting patients received the first dose of UMSC01 through IC injection 4-5 days after STEMI followed by the second dose of UMSC01 via IV infusion 2 days later. The primary endpoint was occurrence of any treatment-related adverse events and the secondary endpoint was changes of serum biomarkers and heart function by cardiac magnetic resonance imaging during a 12-month follow-up period.
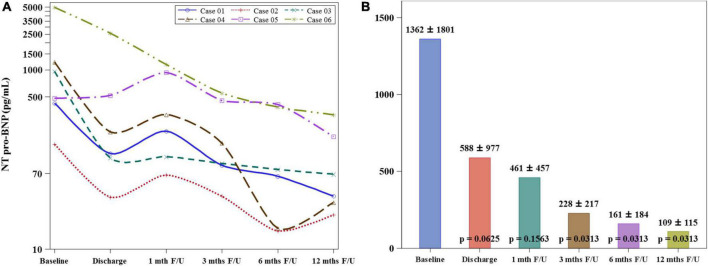
Results: Eight patients gave informed consents, of whom six completed the study. None of the subjects experienced treatment-related serious adverse events or major adverse cardiovascular events during IC or IV infusion of UMSC01 and during the follow-up period. The NT-proBNP level decreased (1362 ± 1801 vs. 109 ± 115 pg/mL, p = 0.0313), the LVEF increased (52.67 ± 12.75% vs. 62.47 ± 17.35%, p = 0.0246), and the wall motion score decreased (26.33 ± 5.57 vs. 22.33 ± 5.85, p = 0.0180) at the 12-month follow-up compared to the baseline values. The serial changes of LVEF were 0.67 ± 3.98, 8.09 ± 6.18, 9.04 ± 10.91, and 9.80 ± 7.56 at 1, 3, 6, and 12 months, respectively as compared to the baseline.
Conclusion: This pilot study shows that combined IC and IV transplantation of UMSC01 in STEMI patients with impaired LVEF appears to be safe, feasible, and potentially beneficial in improving heart function. Further phase 2 studies are required to explore the effectiveness of dual-route transplantation of UMSC01 in STEMI patients.
Keywords: acute myocardial infarction; human pilot trial; intracoronary; intravenous; umbilical mesenchymal stem cell.
Copyright © 2022 Hsiao, Lin, Shyu, Ho, Lu, Chang, Wang, Chen, Lu, Wu, Li, Lin, Tseng, Su, Hsu, Tsai, Chiu, Chen, Lin, Hu, Cho, Tsai, Chang and Jeng.
Conflict of interest statement
C-HT was the founder of Ever Supreme Bio Technology. W-CS, D-YC, K-CC, and L-BJ were stockholders of the Ever Supreme Bio Technology. W-CS was employed by Ever Supreme Bio Technology and China Medical University Hospital. C-TH, C-KT, L-TC, and C-LC were employed by Ever Supreme Bio Technology. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Medical
Research Materials