

The Clinical and Economic Burden of Tardive Dyskinesia in Israel: Real-World Data Analysis
- PMID: 36018237
- PMCID: PMC9426751
- DOI: 10.1097/JCP.0000000000001597
The Clinical and Economic Burden of Tardive Dyskinesia in Israel: Real-World Data Analysis
Abstract
Purpose/background: Tardive dyskinesia (TD) is a hyperkinetic movement disorder caused by exposure to dopamine-receptor blockers. Data on TD burden in Israel are scarce. This analysis assesses the clinical and economic burden of TD in Israeli patients.
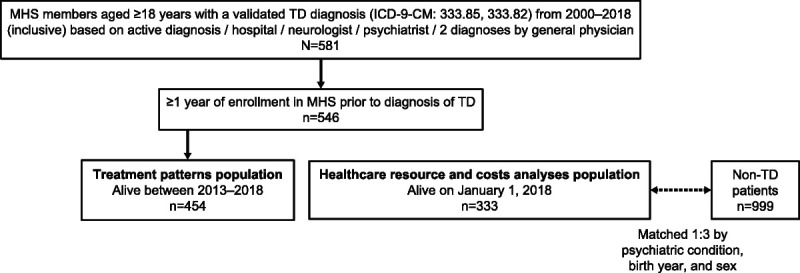
Methods/procedures: This retrospective analysis used a national health plan database (Maccabi Healthcare Services), representing 25% of the Israeli population. The study included adults alive at index date with an International Classification of Diseases, Ninth Revision, Clinical Modification TD diagnosis before 2018 and more than or equal to 1-year enrollment before diagnosis. Tardive dyskinesia patients were matched to non-TD patients (1:3) by underlying psychiatric condition, birth year, and sex. Treatment patterns and 2018 annual health care resource utilization and costs were assessed.
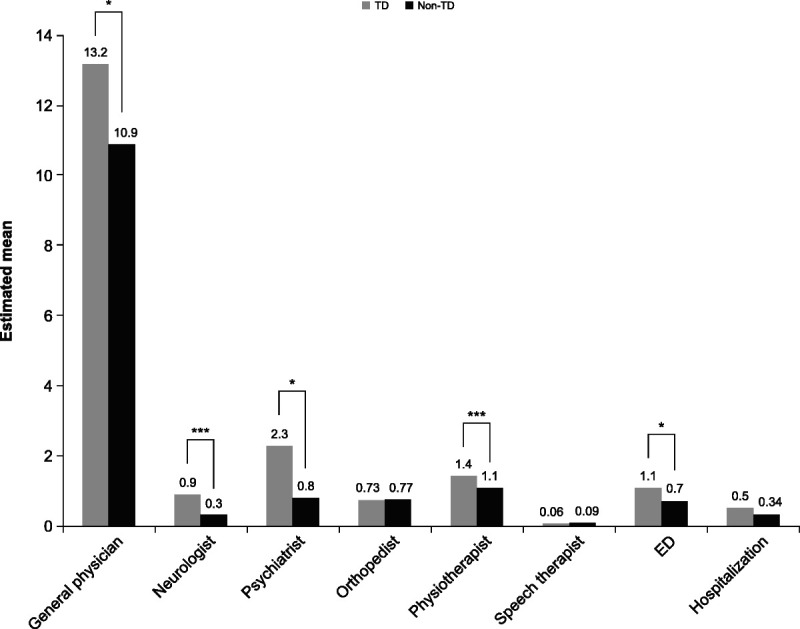
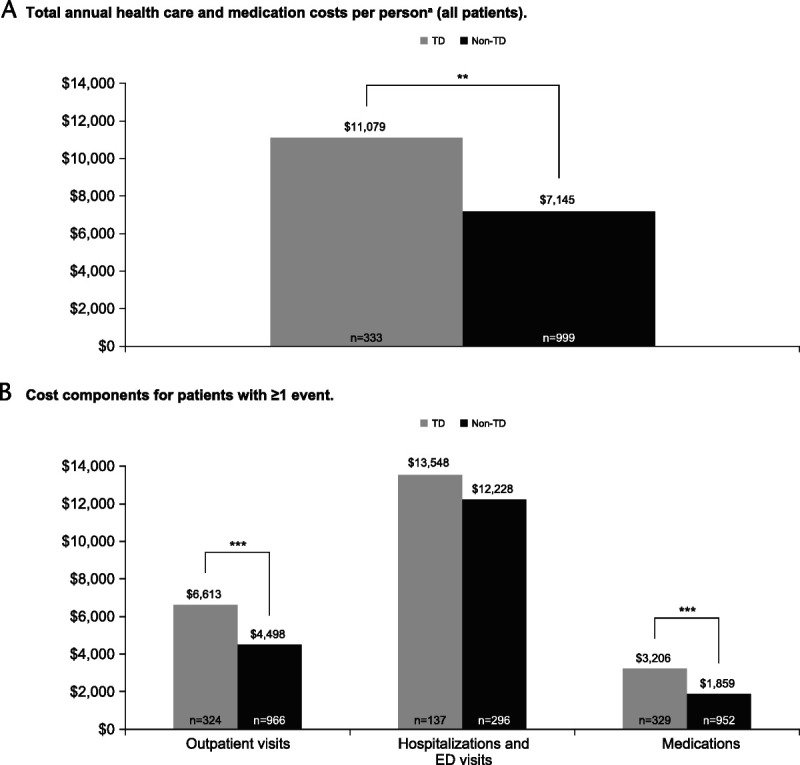
Findings/results: Of 454 TD patients alive between 2013 and 2018, 333 alive on January 1, 2018, were matched to 999 non-TD patients. At baseline, TD patients had lower socioeconomic status and higher proportion of chronic kidney disease and antipsychotic medication use; all analyses were adjusted accordingly. Tardive dyskinesia patients had significantly more visits to general physicians, neurologists, psychiatrists, physiotherapists, and emergency departments versus non-TD patients (all P < 0.05). Tardive dyskinesia patients also had significantly longer hospital stays than non-TD patients ( P = 0.003). Total healthcare and medication costs per patient were significantly higher in the TD versus non-TD population (US $11,079 vs US $7145, P = 0.018).
Implications/conclusions: Israeli TD patients have higher clinical and economic burden than non-TD patients. Understanding real-world health care resource utilization and costs allows clinicians and decision makers to quantify TD burden and prioritize resources for TD patients' treatment.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Figures
Similar articles
-
Health Care Resource Utilization and Costs for Patients with Tardive Dyskinesia.J Manag Care Spec Pharm. 2019 Jul;25(7):810-816. doi: 10.18553/jmcp.2019.25.7.810. J Manag Care Spec Pharm. 2019. PMID: 31232207 Free PMC article.
-
Cumulative Burden of Illness in Veterans With Tardive Dyskinesia and Serious Mental Disorders.J Clin Psychopharmacol. 2020 Jan/Feb;40(1):38-45. doi: 10.1097/JCP.0000000000001142. J Clin Psychopharmacol. 2020. PMID: 31834084
-
The burden of tardive dyskinesia secondary to antipsychotic medication use among patients with mental disorders.Curr Med Res Opin. 2019 Jul;35(7):1205-1214. doi: 10.1080/03007995.2019.1569871. Epub 2019 Feb 15. Curr Med Res Opin. 2019. PMID: 30638073
-
[Prevention and treatment of tardive dyskinesia caused by antipsychotic drugs].Encephale. 2016 Jun;42(3):248-54. doi: 10.1016/j.encep.2015.12.021. Epub 2016 Feb 26. Encephale. 2016. PMID: 26922134 Review. French.
-
Tardive dyskinesia: Who gets it and why.Parkinsonism Relat Disord. 2019 Feb;59:151-154. doi: 10.1016/j.parkreldis.2018.11.017. Epub 2018 Nov 15. Parkinsonism Relat Disord. 2019. PMID: 30522959 Review.
Cited by
-
Unique and overlapping mechanisms of valbenazine, deutetrabenazine, and vitamin E for tardive dyskinesia.Schizophrenia (Heidelb). 2025 Apr 23;11(1):69. doi: 10.1038/s41537-025-00618-w. Schizophrenia (Heidelb). 2025. PMID: 40268947 Free PMC article.
-
Operationalising routinely collected patient data in research to further the pursuit of social justice and health equity: a team-based scoping review.BMC Med Res Methodol. 2025 Jan 21;25(1):14. doi: 10.1186/s12874-025-02466-9. BMC Med Res Methodol. 2025. PMID: 39838312 Free PMC article.
References
-
- Lerner PP, Miodownik C, Lerner V. Tardive dyskinesia (syndrome): current concept and modern approaches to its management. Psychiatry Clin Neurosci. 2015;69:321–334. - PubMed
-
- Jain R, Correll CU. Tardive dyskinesia: recognition, patient assessment, and differential diagnosis. J Clin Psychiatry. 2018;79:nu17034ah1c. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
