

Pulmonary Hypertension in Children with Down Syndrome: Results from the Pediatric Pulmonary Hypertension Network Registry
- PMID: 36027975
- PMCID: PMC10195185
- DOI: 10.1016/j.jpeds.2022.08.027
Pulmonary Hypertension in Children with Down Syndrome: Results from the Pediatric Pulmonary Hypertension Network Registry
Abstract
Objective: To characterize distinct comorbidities, outcomes, and treatment patterns in children with Down syndrome and pulmonary hypertension in a large, multicenter pediatric pulmonary hypertension registry.
Study design: We analyzed data from the Pediatric Pulmonary Hypertension Network (PPHNet) Registry, comparing demographic and clinical characteristics of children with Down syndrome and children without Down syndrome. We examined factors associated with pulmonary hypertension resolution and a composite outcome of pulmonary hypertension severity in the cohort with Down syndrome.
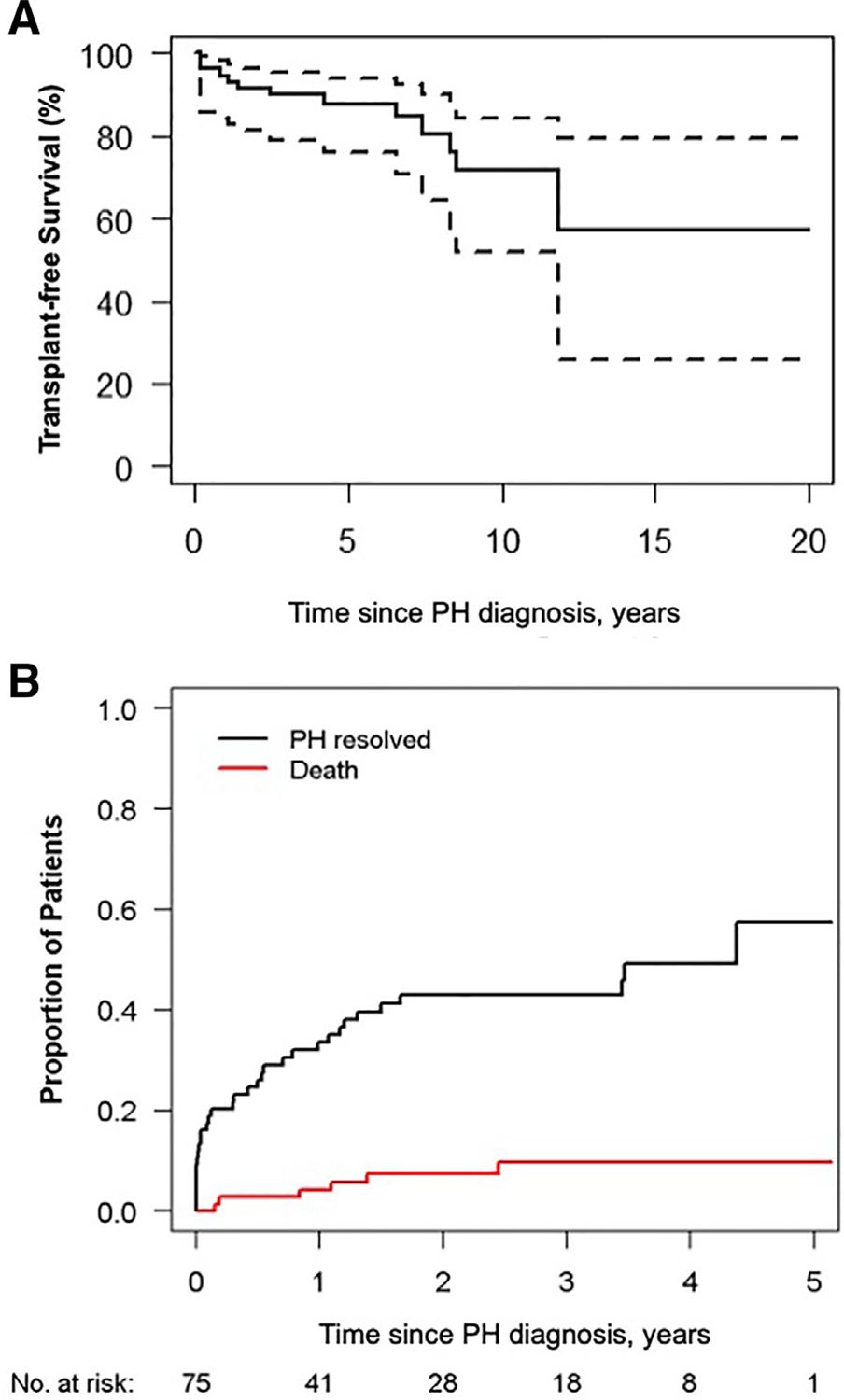
Results: Of 1475 pediatric patients with pulmonary hypertension, 158 (11%) had Down syndrome. The median age at diagnosis of pulmonary hypertension in patients with Down syndrome was 0.49 year (IQR, 0.21-1.77 years), similar to that in patients without Down syndrome. There was no difference in rates of cardiac catheterization and prescribed pulmonary hypertension medications in children with Down syndrome and those without Down syndrome. Comorbidities in Down syndrome included congenital heart disease (95%; repaired in 68%), sleep apnea (56%), prematurity (49%), recurrent respiratory exacerbations (35%), gastroesophageal reflux (38%), and aspiration (31%). Pulmonary hypertension resolved in 43% after 3 years, associated with a diagnosis of pulmonary hypertension at age <6 months (54% vs 29%; P = .002) and a pretricuspid shunt (65% vs 38%; P = .02). Five-year transplantation-free survival was 88% (95% CI, 80%-97%). Tracheostomy (hazard ratio [HR], 3.29; 95% CI, 1.61-6.69) and reflux medication use (HR, 2.08; 95% CI, 1.11-3.90) were independently associated with a composite outcome of severe pulmonary hypertension.
Conclusions: Despite high rates of cardiac and respiratory comorbidities that influence the severity of pulmonary hypertension, children with Down syndrome-associated pulmonary hypertension generally have a survival rate similar to that of children with non-Down syndrome-associated pulmonary hypertension. Resolution of pulmonary hypertension is common but reduced in children with complicated respiratory comorbidities.
Keywords: Down syndrome; congenital heart disease; developmental lung disease; pediatric pulmonary hypertension; pulmonary vascular disease.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
