

Self-report of chronic diseases in old-aged individuals: extent of agreement with general practitioner medical records in the German AugUR study
- PMID: 36028306
- PMCID: PMC9554083
- DOI: 10.1136/jech-2022-219096
Self-report of chronic diseases in old-aged individuals: extent of agreement with general practitioner medical records in the German AugUR study
Abstract
Background: To estimate prevalence and incidence of diseases through self-reports in observational studies, it is important to understand the accuracy of participant reports. We aimed to quantify the agreement of self-reported and general practitioner-reported diseases in an old-aged population and to identify socio-demographic determinants of agreement.
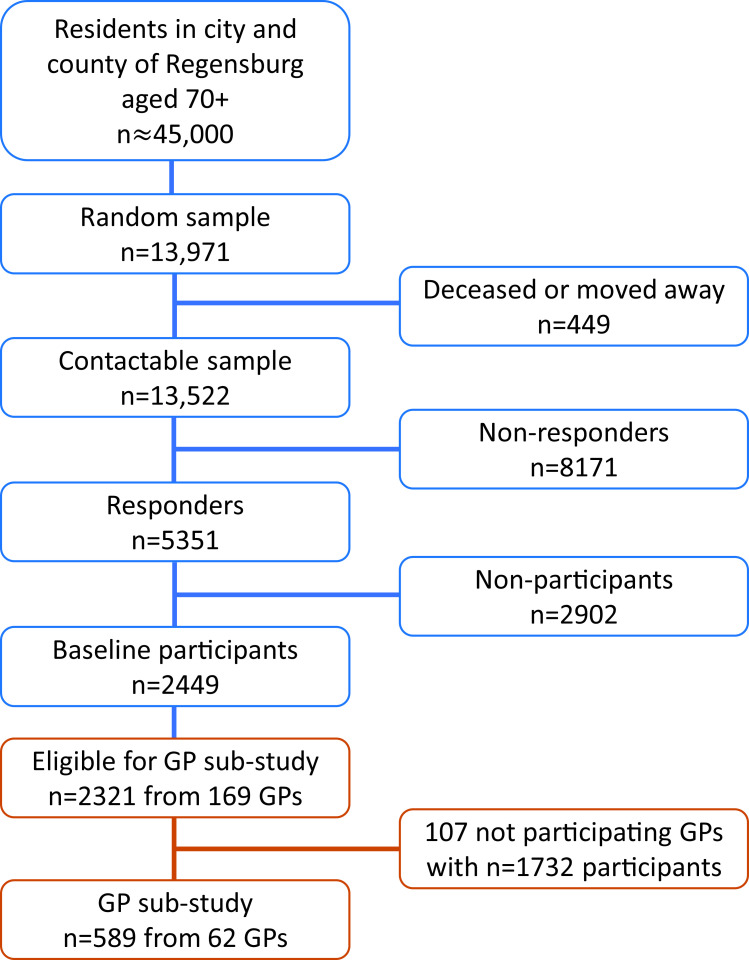
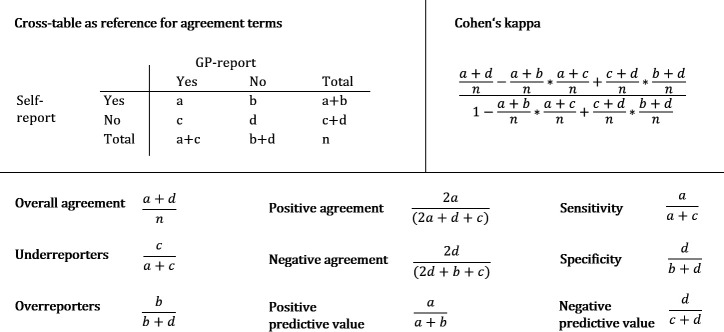
Methods: This analysis was conducted as part of the AugUR study (n=2449), a prospective population-based cohort study in individuals aged 70-95 years, including 2321 participants with consent to contact physicians. Self-reported chronic diseases of participants were compared with medical data provided by their respective general practitioners (n=589, response rate=25.4%). We derived overall agreement, over-reporting/under-reporting, and Cohen's kappa and used logistic regression to evaluate the dependency of agreement on participants' sociodemographic characteristics.
Results: Among the 589 participants (53.1% women), 96.9% reported at least one of the evaluated chronic diseases. Overall agreement was >80% for hypertension, diabetes, myocardial infarction, stroke, cancer, asthma, bronchitis/chronic obstructive pulmonary disease and rheumatoid arthritis, but lower for heart failure, kidney disease and arthrosis. Cohen's kappa was highest for diabetes and cancer and lowest for heart failure, musculoskeletal, kidney and lung diseases. Sex was the primary determinant of agreement on stroke, kidney disease, cancer and rheumatoid arthritis. Agreement for myocardial infarction and stroke was most compromised by older age and for cancer by lower educational level.
Conclusion: Self-reports may be an effective tool to assess diabetes and cancer in observational studies in the old and very old aged. In contrast, self-reports on heart failure, musculoskeletal, kidney or lung diseases may be substantially imprecise.
Keywords: AGING; EPIDEMIOLOGY; GENERAL PRACTICE; GERIATRICS; HEALTH STATUS.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Cardiac late events in German breast cancer patients: a validation study on the agreement between patient self-reports and information from physicians.BMC Cardiovasc Disord. 2018 Nov 29;18(1):218. doi: 10.1186/s12872-018-0961-7. BMC Cardiovasc Disord. 2018. PMID: 30497402 Free PMC article.
-
Self-reports and general practitioner information on the presence of chronic diseases in community dwelling elderly. A study on the accuracy of patients' self-reports and on determinants of inaccuracy.J Clin Epidemiol. 1996 Dec;49(12):1407-17. doi: 10.1016/s0895-4356(96)00274-0. J Clin Epidemiol. 1996. PMID: 8970491
-
Agreement between self-reported and general practitioner-reported chronic conditions among multimorbid patients in primary care - results of the MultiCare Cohort Study.BMC Fam Pract. 2014 Mar 1;15:39. doi: 10.1186/1471-2296-15-39. BMC Fam Pract. 2014. PMID: 24580758 Free PMC article.
-
Agreement between self-reported diseases from health surveys and national health registry data: a Danish nationwide study.J Epidemiol Community Health. 2023 Feb;77(2):116-122. doi: 10.1136/jech-2022-219944. Epub 2022 Nov 29. J Epidemiol Community Health. 2023. PMID: 36446554
-
Identification of diabetes, heart disease, hypertension and stroke in mid- and older-aged women: Comparing self-report and administrative hospital data records.Geriatr Gerontol Int. 2016 Jan;16(1):95-102. doi: 10.1111/ggi.12442. Epub 2015 Jan 22. Geriatr Gerontol Int. 2016. PMID: 25613080
Cited by
-
Healthy lifestyle and cognitive decline in middle-aged and older adults residing in 14 European countries.Nat Commun. 2024 Jun 27;15(1):5003. doi: 10.1038/s41467-024-49262-5. Nat Commun. 2024. PMID: 38937442 Free PMC article.
-
Diabetes and Hypertension at Midlife Predict Increases in Biomarkers of Dementia Among Black Americans.J Racial Ethn Health Disparities. 2025 Feb 28. doi: 10.1007/s40615-025-02310-2. Online ahead of print. J Racial Ethn Health Disparities. 2025. PMID: 40021611
-
A comparison between the self-report of chronic cardiovascular diseases with health insurance data: insights from the population-based LIFE-Adult study.Arch Public Health. 2025 May 7;83(1):124. doi: 10.1186/s13690-025-01606-3. Arch Public Health. 2025. PMID: 40336119 Free PMC article.
-
Reliability and Validity of Self-Reported Vascular Risk Factors: Hypertension, Diabetes, and Heart Disease, in a Multi-Ethnic Community Based Study of Aging and Dementia.J Alzheimers Dis. 2023;95(1):275-285. doi: 10.3233/JAD-230374. J Alzheimers Dis. 2023. PMID: 37483004 Free PMC article.
-
Validation of self-reported morbidities in the Korean Atomic Bomb Survivor Cohort.Epidemiol Health. 2024;46:e2024058. doi: 10.4178/epih.e2024058. Epub 2024 Jun 28. Epidemiol Health. 2024. PMID: 38993111 Free PMC article.
References
LinkOut - more resources
Full Text Sources