

The CCTG PA.7 phase II trial of gemcitabine and nab-paclitaxel with or without durvalumab and tremelimumab as initial therapy in metastatic pancreatic ductal adenocarcinoma
- PMID: 36028483
- PMCID: PMC9418247
- DOI: 10.1038/s41467-022-32591-8
The CCTG PA.7 phase II trial of gemcitabine and nab-paclitaxel with or without durvalumab and tremelimumab as initial therapy in metastatic pancreatic ductal adenocarcinoma
Abstract
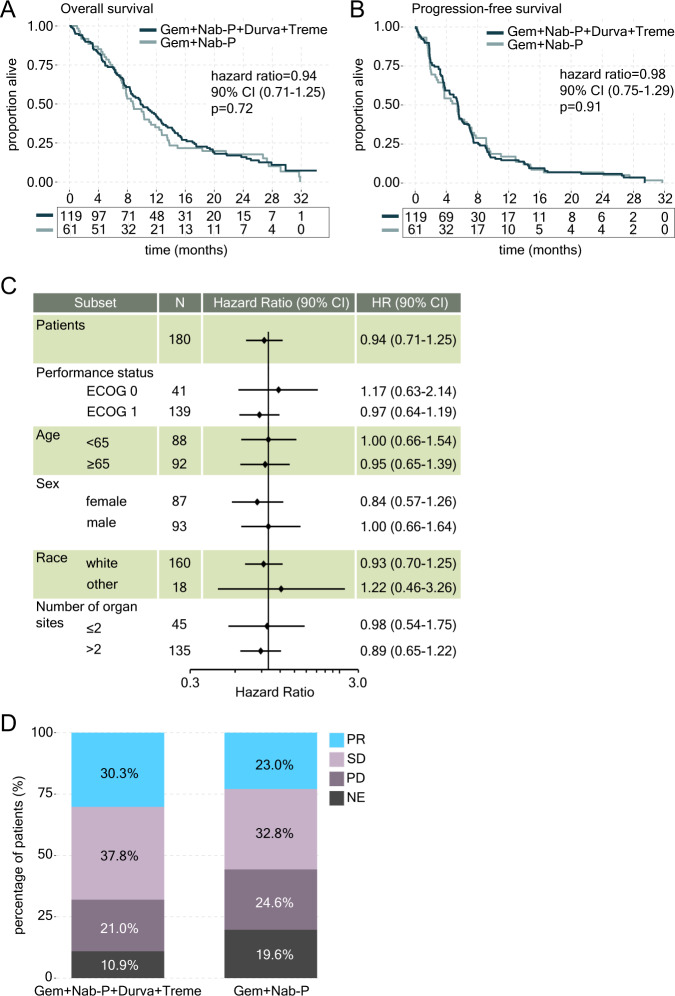
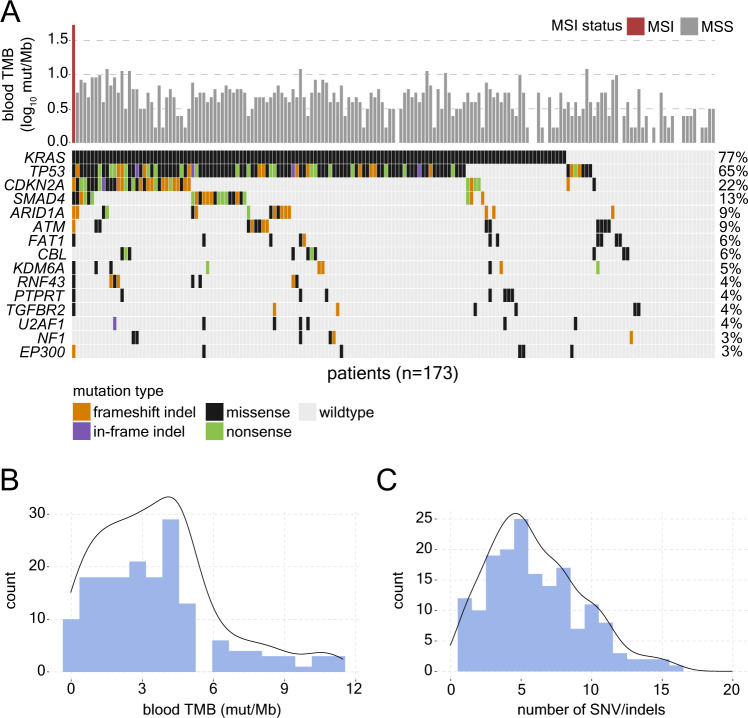
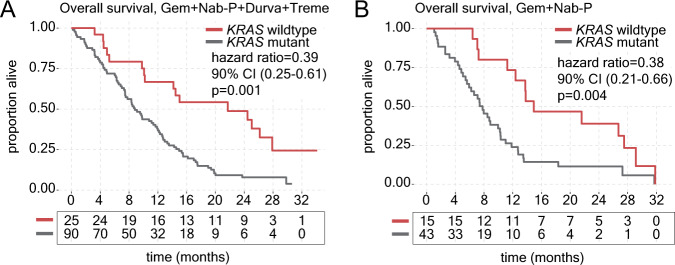
Immunotherapy-based monotherapy treatment in metastatic pancreatic ductal adenocarcinoma (mPDAC) has shown limited benefit outside of the mismatch repair deficiency setting, while safety and efficacy of combining dual-checkpoint inhibitor immunotherapy with chemotherapy remains uncertain. Here, we present results from the CCTG PA.7 study (NCT02879318), a randomized phase II trial comparing gemcitabine and nab-paclitaxel with and without immune checkpoint inhibitors durvalumab and tremelimumab in 180 patients with mPDAC. The primary endpoint was overall survival. Secondary endpoints included progression-free survival and objective response rate. Results of the trial were negative as combination immunotherapy did not improve survival among the unselected patient population (p = 0.72) and toxicity was limited to elevation of lymphocytes in the combination immunotherapy group (p = 0.02). Exploratory baseline circulating tumor DNA (ctDNA) sequencing revealed increased survival for patients with KRAS wildtype tumors in both the combination immunotherapy (p = 0.001) and chemotherapy (p = 0.004) groups. These data support the utility of ctDNA analysis in PDAC and the prognostic value of ctDNA-based KRAS mutation status.
© 2022. The Author(s).
Conflict of interest statement
P.D. and S.J. are employees of Predicine. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
